

Almost one-third of our lives is spent in the workplace, where much of our interaction with others takes place and where we are exposed to stressful situations. Work-related stress has consequences for the individual's physical and mental health. Stress and professional burnout syndrome are the main consequences of work situations characterized by a constant state of tension. Stress is the second leading cause of absenteeism in the European Union, and around 12% of European workers are currently affected by burnout syndrome. It is therefore vital to identify demotivated and stressed staff in both large organizations (hospitals and clinics) and smaller centers (private practices) so as to facilitate preventive measures and ensure early intervention in situations of stress, with a view to improving the performance of work teams.
Las personas invertimos casi un tercio de nuestra vida en el lugar de trabajo, donde se desarrollan gran parte de las relaciones interpersonales y las situaciones de tensión. El estrés laboral asociado a estas conlleva consecuencias para la salud física y mental de las personas. El estrés laboral y el síndrome del profesional quemado (burnout) son las principales consecuencias derivadas de las situaciones de tensión constantes en el trabajo. El estrés es la segunda causa de baja laboral en la Unión Europea, y alrededor de un 12% de los trabajadores europeos podría padecer actualmente el síndrome del profesional quemado. Por todo esto, es fundamental la detección en las organizaciones, grandes (hospitales y clínicas) y pequeñas (consultas), del personal desmotivado y estresado, ya que permitirá una prevención e intervención precoz en las situaciones de tensión generadas y una mejora en el funcionamiento de los equipos de trabajo.
People spend almost a third of their lives at work. The workplace is where many of our interpersonal relationships are developed and where our vital interests are channeled. Work is therefore one of the key activities of human beings, and stressful situations at work and work-related stress are among the most important consequences for people's physical and mental health.
Work-Related StressStress is defined as a relationship or transaction in terms of adaptation and interaction between a person and the setting or environment that can place a burden on individual well-being and lead to psychological disorders, unhealthy conducts, and, ultimately, disease.1 Stress can be a consequence of multiple factors and circumstances. However, due to its importance in people's lives, the world of work is one of the main generators of stress.2 Therefore, stress must be understood as an interactive problem involving both the worker and the organization.
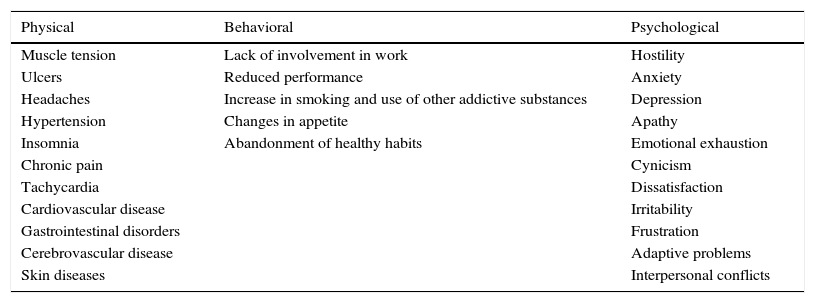
Work-related stress has important consequences both for people (Table 1) and for organizations. Many studies have demonstrated the relationships between stress and health.3–5 In dermatology, for example, psychosocially induced stress can trigger or exacerbate numerous skin diseases, including rosacea, lichen planus, various types of eczema including seborrheic dermatitis, psoriasis, and many others.6,7 Stress is one of the main risk factors for heart disease, stroke, chronic pain, etc. It plays a role in the appearance of burnout syndrome8 and is linked to workplace harassment (or “mobbing”)9 and adaptive disorders.10 It also affects quality of life in general.11
Health Impact of Stressful Situations at Work.
| Physical | Behavioral | Psychological |
|---|---|---|
| Muscle tension | Lack of involvement in work | Hostility |
| Ulcers | Reduced performance | Anxiety |
| Headaches | Increase in smoking and use of other addictive substances | Depression |
| Hypertension | Changes in appetite | Apathy |
| Insomnia | Abandonment of healthy habits | Emotional exhaustion |
| Chronic pain | Cynicism | |
| Tachycardia | Dissatisfaction | |
| Cardiovascular disease | Irritability | |
| Gastrointestinal disorders | Frustration | |
| Cerebrovascular disease | Adaptive problems | |
| Skin diseases | Interpersonal conflicts |
Burnout syndrome develops as a result of situations of chronic work-related stress. According to Maslach and Jackson,12 burnout syndrome affects workers’ emotional responses and includes symptoms such as emotional exhaustion, depersonalization, and low personal accomplishment. Emotional exhaustion, which refers to the progressive loss of the capacity to dedicate oneself to work, represents an individual dimension of burnout. Depersonalization pertains to the worker's interpersonal context and entails distancing oneself emotionally from the users of one's services by adopting impersonal, insensitive, or hardened behaviors. Low personal accomplishment occurs in professionally disgruntled, unmotivated, and unsatisfied workers as a result of a negative assessment of one's achievements and dissatisfaction with one's job.
This definition of burnout syndrome, initially developed to cover care and service professions, was reconceptualized to improve its validity and to make it applicable to all types of occupations. Burnout syndrome is now defined as “a prolonged response to chronic emotional and interpersonal stressors on the job, and is determined by the three dimensions of exhaustion, cynicism, and inefficacy.”13 Exhaustion is defined as the feeling of not being able to give any more of oneself emotionally as a consequence of prolonged exposure to work-related demands. Cynicism refers to a lack of interest and a loss of meaning, as well as indifference and the distancing of oneself from one's job. Inefficacy is a perception of not performing tasks adequately and a feeling of incompetence in one's assigned post.
A new and more extensive definition of burnout proposes a classification of the syndrome in 3 clinical subtypes. The “frenetic” subtype is seen in highly involved, ambitious, overloaded people who work increasingly harder until they reach the point of exhaustion. The “under-challenged” subtype is seen in workers who face insufficient challenges and are indifferent, unsatisfied, bored, lack personal development in their jobs, and have to cope with unstimulating work conditions. The “worn-out” subtype—characterized by a feeling of not being able to control results, lack of recognition for one's efforts, and neglect of responsibilities—is seen in people who immediately give up when faced with stress or the absence of gratification.14,15
The consensus view is that the following factors favor the development of burnout syndrome: personal characteristics (age, sex, personality), social characteristics (marital status, number of children), and job characteristics (work overload, relationships with team members, seniority, shift, type of activity).16
The development of burnout syndrome in a worker is a gradual process. The syndrome develops continuously, with fluctuations over time, such that milder and more acute phases may appear. Depending on the preventive measures or interventions carried out, the symptoms can either become more acute or stabilize and even subside.16
As Table 2 indicates, burnout syndrome has very negative consequences. Burnout can affect people's physical and/or mental health, giving rise to psychosomatic disorders such as cutaneous and mucosal alterations, cardiorespiratory abnormalities, headaches, etc., and psychopathological disorders such as anxiety, obsessive-compulsive behaviors, depression, and addictions. In organizations, burnout can cause a severe reduction in professional performance, a decline in the quality of care or services, high turnover, absenteeism, and even job abandonment. Professionals in the education and health fields are exposed to especially high risk of burnout syndrome. Dermatologists, like other specialists, are no exception. Renzi et al.17 studied burnout and job satisfaction in dermatologists and nurses working with dermatology patients as compared to physicians and nurses in other specialties at a hospital in Rome. The authors distributed a questionnaire to the respective groups. The results showed a) that burnout was similar in dermatologists and other specialists, and b) that nurses at the general hospital were more likely than their counterparts at the dermatology hospital to experience burnout and were less satisfied with the management of their units and with their professional development opportunities. In another study, Olkinuora et al.18 analyzed stress symptoms, burnout, and suicidal ideation in 2671 Finnish medical workers. In male specialists, the highest burnout indices were observed in general practice, psychiatry, internal medicine, oncology, pulmonary diseases, and—surprisingly—dermatology. In female specialists, the highest indices were seen in general practice, radiology, internal medicine, neurology, pulmonary diseases, and—again—dermatology. Non-specialists had a higher risk of burnout than specialists of both sexes. Additionally, higher burnout rates were observed in physicians working at municipal health centers than in those who worked at private centers, universities, or research institutes. The authors distinguished between higher-burnout specialties such as oncology, pulmonary diseases, and psychiatry and lower-burnout specialties such as obstetrics, gynecology, otorhinolaryngology, and ophthalmology. A third study, carried out in Croatia, studied the prevalence of burnout in doctors in 3 specialty groups: a) internal medicine and pediatrics, b) surgery and obstetrics/gynecology, and c) dermatology, otorhinolaryngology, and ophthalmology. Fortunately, 81.86% of the specialists analyzed had no symptoms of burnout. Among those who did have burnout, there were no differences by sex, number of work hours, or specialty group.19
Symptoms Associated With Burnout Syndrome.
| Physical | Emotional |
| Headaches | Emotional distancing |
| Insomnia | Cynical attitude and apathy |
| Osteomuscular pain | Helplessness |
| Gastrointestinal abnormalities | Impatience and irritability |
| Cardiac abnormalities | Disorientation |
| Chronic fatigue | Depression |
| Psychological | Work-related |
| Feelings of emptiness, exhaustion, failure and powerlessness | Decrease in work capacity |
| Low self-esteem and professional fulfillment | Over- or under-involvement and motivation |
| Nervousness and restlessness | Boredom and presenteeism |
| Loss of values and expectations | Decrease in quality of work |
| Modification of self-concept | Hostility |
| Difficulty concentrating | Interpersonal conflicts |
| Low tolerance of frustration | Communication problems |
| Aggressiveness | |
| Behavioral | |
| Addictive and avoidance behaviors | |
| Inability to lead a relaxed life | |
| High-risk behaviors | |
| Increasing irritability and low personal performance | |
| Disorganization | |
According to surveys on the conditions of quality of life at work in the European Union, stress is the second most common reason for sick leave in the region.20 The surveys also found that 28% of workers suffered from stress21; in 2005, following the incorporation of new European Union member states, this figure rose to 30%.22 The prevalence of burnout syndrome is directly related to work-related stress and ranges from 4%23 to 30.5%.24 In general, it is considered that around 12% of European workers could currently have burnout syndrome. In the health sector specifically, the prevalence of burnout syndrome has been estimated at around 14.9% in various European countries, including Spain.25 Stress is considered to be one of the risk factors that contributes the most to morbidity and mortality in any working population, and it is therefore among the factors that contribute the most to health problems in the general population.23
Managing Stressful SituationsWork-related stress and burnout syndrome constitute a psychological, physical, and biological reaction that can affect both professionals and patients. Stress must therefore be taken into account in medical facilities, especially in dermatology clinics, where stress is one of the situations most closely related to the onset, exacerbation, and perpetuation of skin diseases. Skin diseases of this type often cause severe physical and psychological suffering and have a greater impact on patients’ quality of life. Consequently, providing care for these patients in dermatology clinics can be very difficult. The diseases they present can be very difficult to treat because of their characteristics and consequences.17 In dermatology, the assessment of emotional balance is an important element in the diagnosis, treatment, and prevention of numerous diseases. Stress must therefore be taken into account because it can be related to morbidity associated with skin conditions in a working population.26
With regard to controlling situations of strain and stress, as in other diseases, there are 3 types of prevention27:
- •
Primary intervention: This type of intervention focuses on reducing or eliminating the causes of stress through activities aimed at promoting mental health in the workplace and adapting the work environment. The aim of these interventions is to create a healthier work environment.
- •
Secondary intervention: The aim of this type of intervention is to reduce the health-related consequences of stress through actions that lead to greater awareness and the adoption of effective coping strategies, thereby strengthening workers’ skills and capacities.
- •
Tertiary intervention: These interventions focus on treating people in whom the consequences of work-related stress have been or are currently present. The aim of this type of intervention is to reduce the negative consequences of stress in order to rehabilitate and readjust the person and to facilitate his or her return to work.
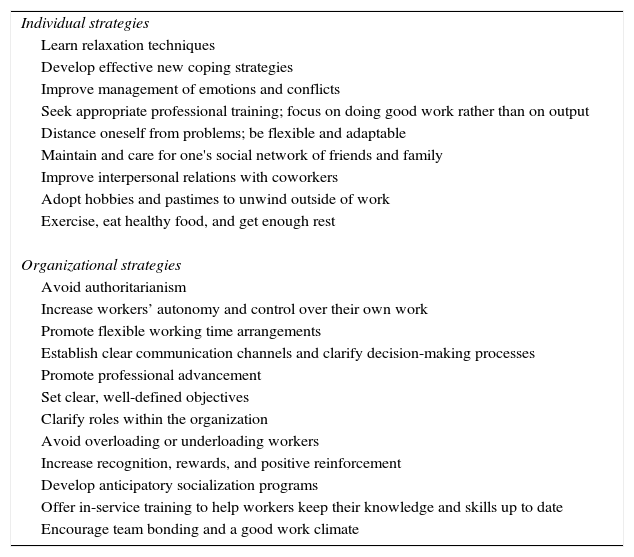
In addition, a series of individual and organizational strategies can be implemented by workers as well as organizations—either large (hospitals) or small (dermatologists’ offices)—in order to prevent and reduce stressful situations that generate work-related stress, which in the long term leads to the development of burnout syndrome16 (Table 3).
Individual and Organizational Strategies to Prevent and Reduce Stressful Situations That Cause Work-Related Stress.
| Individual strategies |
| Learn relaxation techniques |
| Develop effective new coping strategies |
| Improve management of emotions and conflicts |
| Seek appropriate professional training; focus on doing good work rather than on output |
| Distance oneself from problems; be flexible and adaptable |
| Maintain and care for one's social network of friends and family |
| Improve interpersonal relations with coworkers |
| Adopt hobbies and pastimes to unwind outside of work |
| Exercise, eat healthy food, and get enough rest |
| Organizational strategies |
| Avoid authoritarianism |
| Increase workers’ autonomy and control over their own work |
| Promote flexible working time arrangements |
| Establish clear communication channels and clarify decision-making processes |
| Promote professional advancement |
| Set clear, well-defined objectives |
| Clarify roles within the organization |
| Avoid overloading or underloading workers |
| Increase recognition, rewards, and positive reinforcement |
| Develop anticipatory socialization programs |
| Offer in-service training to help workers keep their knowledge and skills up to date |
| Encourage team bonding and a good work climate |
The work climate is the set of all people, groups, organizations, and physical or social elements with which the organization shares information, results, products, etc.28 In order to improve the achievement of goals and objectives and reduce stressful situations, organizations should foster a climate in which workers feel comfortable, involved, and integrated, with good relationships both horizontally (with coworkers) and vertically (with superiors). A good work climate has positive consequences such as accomplishment, affiliation, power, productivity, low turnover, satisfaction, involvement, adaptation, innovation, etc. In contrast, an inappropriate work climate causes high turnover, absenteeism, low levels of innovation, low productivity, etc.16
In order to improve the work climate, organizations should implement strategies to reduce stressful situations and increase workers’ commitment to and involvement in the company—or the hospital, in our case—thereby creating in the workers a sense of belonging and aligning the organization's objective with the workers’ personal objectives, increasing workers’ motivation and satisfaction, and fostering mutual cooperation, support, and assistance, both horizontally (among coworkers) and vertically (from managers to employees).
Teams arise from previously formed groups. We understand a “group” to be a set of interdependent individuals who share a common destiny, in the sense that something that affects one group member will also affect the others.29 Due to this shared objective, the relationship between these individuals must be based on cooperation, as they are interdependent and responsible for everything that happens. A group becomes a team when, in addition to a shared sense of commitment, it also pursues important group-based performance outcomes or results.30 In other words, teams have a purpose that is oriented towards achieving particular objectives.
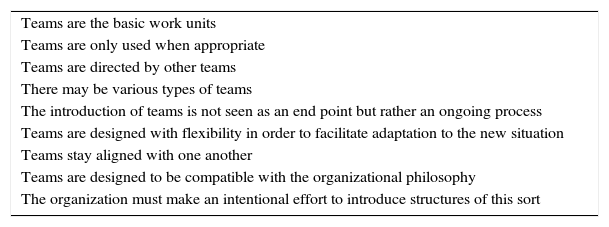
Table 4 shows the characteristics that are common to all team-based organizations. When an organization such as a clinic or a hospital has adequate teams, it results in lower costs (both direct and indirect), better mechanisms for coordinating and integrating members, and greater creativity. In addition, teams also produce emotional and psychological benefits for their members because they satisfy various individual needs as well as the need for affiliation and integration in a group.31 This enables workers—administrative staff, hospital porters, surgeons, traumatologists, dermatologists, nurses, etc.—to have greater autonomy and responsibility and therefore achieve more ambitious targets and objectives.
Characteristics of a Team-Based Organization.
| Teams are the basic work units |
| Teams are only used when appropriate |
| Teams are directed by other teams |
| There may be various types of teams |
| The introduction of teams is not seen as an end point but rather an ongoing process |
| Teams are designed with flexibility in order to facilitate adaptation to the new situation |
| Teams stay aligned with one another |
| Teams are designed to be compatible with the organizational philosophy |
| The organization must make an intentional effort to introduce structures of this sort |
In hospitals and clinics, is very common for work to be done by multidisciplinary teams consisting of professionals from different fields and schools of thought. As a result, these teams are more vulnerable to conflict. The ability to manage conflicts is essential to the proper functioning of a team. The aim is not to avoid conflicts, but rather to resolve them effectively and prevent negative effects. A conflict is a discrepancy and contradiction that arises as a result of differences between people. Well-resolved conflicts bring about healthy and favorable consequences for both the organization and the people who form part of it. It is important to avoid incorrect conflict management, which can lead to a situation of passivity and stagnation in the group. In contrast, a well-managed conflict gives rise to change, growth, and creativity. Group conflict has been associated with greater innovation and more effective interpersonal relationships,32 but when not managed properly it can also lead to diminished efficacy and well-being as well as higher turnover.33 There are 2 possible types of conflicts34: a) conflicts related to information or tasks, and b) conflicts of interest or emotional and interpersonal conflicts. Conflicts of the first type are valuable because they can prompt members of the team and of the organization to reevaluate the situation and adapt it to their objectives. Conflicts of the second type are always negative for a team.
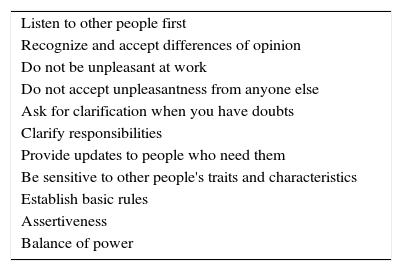
The following is an appropriate way to manage a conflict. Before getting involved, be aware of what the conflict is and what its possible consequences are. Observe, listen, and interpret before acting. It is important to detect and accept the existence of a conflict; ignoring the conflict neither solves it nor eliminates it. Once you have accepted that a conflict exists, identify the people involved and assess the importance of the conflict by observing and listening to the various parties. Then, reach consensus-based decisions about how to solve the conflict with the participation of the involved parties. It is fundamental to observe and show interest in the existing problems in order to address their causes. Table 5 shows a series of basic recommendations to reduce the likelihood of conflict.
Basic Recommendations to Reduce the Likelihood of Conflict.
| Listen to other people first |
| Recognize and accept differences of opinion |
| Do not be unpleasant at work |
| Do not accept unpleasantness from anyone else |
| Ask for clarification when you have doubts |
| Clarify responsibilities |
| Provide updates to people who need them |
| Be sensitive to other people's traits and characteristics |
| Establish basic rules |
| Assertiveness |
| Balance of power |
In order for teams to function properly, there need to be basic rules based on respect, balance of power, values, and equality, in addition to adequate communication and assertive attitudes.
Communication within a team is very important because it is a requirement for the team's success. However, not all types of communication are effective. There are positive types of communication that bring about change and progress, while other types of communication generate negative consequences and a hostile work environment.
Assertiveness—the most appropriate and reinforcing type of behavior—entails having respect for others and asking for respect in return, reaching a compromise between the involved parties, and allowing individuals to express themselves freely and to achieve their objectives. Whereas nonassertive people express their opinions inadequately—either because they avoid expressing opinions in order to please others or because they disrespectfully impose their opinions on others—assertive people express respect for themselves and for others. This, in turn, increases trust and causes people to feel more satisfied with themselves and with their relationships with other people.
By using assertive communication, teams can develop more fluid, frank, and direct communication among their members. In addition, the level of respect for other people will be greater and the work environment will be ideal for achieving shared objectives.
Finally, in large organizations (hospitals and clinics) as well as small facilities (doctor's offices), it is important to detect workers who are unmotivated or stressed in order to allow early prevention and intervention in stressful situations and to improve the functioning of teams.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: García-Campayo J, Puebla-Guedea M, Herrera-Mercadal P, Daudén E. Desmotivación del personal sanitario y síndrome de burnout. Control de las situaciones de tensión. La importancia del trabajo en equipo. Actas Dermosifiliogr. 2016;107:400–406.


