


Blue nevus is considered to be a benign acquired melanocytic nevus with blue pigmentation that results from the accumulation and differentiation of melanocytic cells in the dermis.1 We describe the case of a common blue nevus with satellite lesions that mimicked locally disseminated malignant melanoma. Fewer than 10 such cases have been reported in the literature.2,3
A 57-year-old man with no personal or family history of skin cancer presented at our hospital during the annual skin cancer prevention and detection campaign with tumor lesions on his scalp and forehead. They were asymptomatic and had appeared a year earlier.
Physical examination showed an asymmetric bluish-black tumor lesion with irregular borders and a serosanguineous crust. The lesion measured 16 x 5mm in diameter and was accompanied by satellite guttate lesions with a diameter of 1 to 2mm (Fig. 1). Dermoscopic examination showed a homogeneous blue pattern with shiny white streaks and peripheral serosanguineous crusts (Fig. 2A).


Based on the clinical and dermoscopic findings and with a tentative diagnosis of malignant melanoma, it was decided to perform an excisional biopsy of the largest lesion and a smaller adjacent one. Histologic examination in both cases showed fibrosis and a proliferation of spindle-shaped nevus cells, with marked intracytoplasmic melanin pigmentation and melanophages in the dermis (Fig. 2B). There were no signs of malignancy and a diagnosis of common blue nevus was made.
Blue nevus was first described by Max Tieche in 1906.4 It is considered to be the result of an ectopic accumulation of melanocytes retained in the dermis during migration from the neural crest to the epidermis.5
Blue nevus is usually acquired and it typically presents as a solitary asymptomatic bluish or bluish-black tumor located on the head or neck or on the dorsum of the hands or feet.2,3
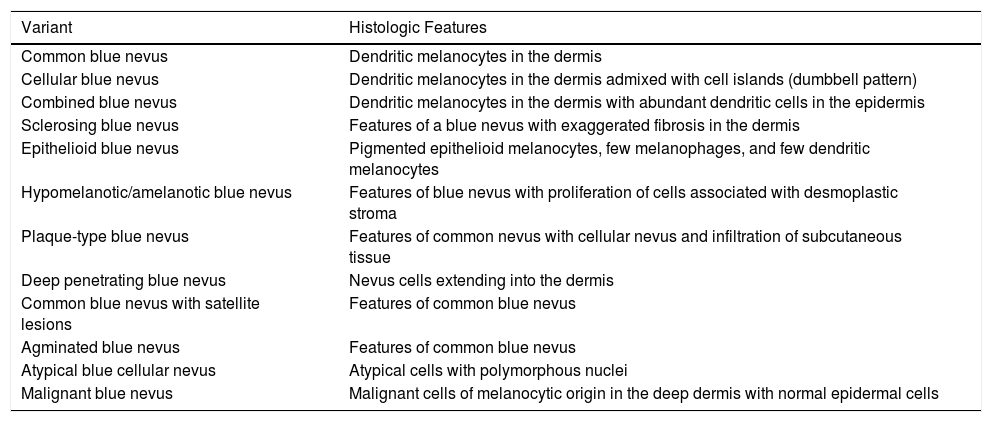
Several clinical and histologic variants have been described (Table 1), the most common of which are common blue nevus, cellular blue nevus, and combined blue nevus.6,7 The variant described herein, blue nevus with satellite lesions clinically mimicking malignant melanoma with cutaneous metastases, is rare.2,7–9 The etiology and pathogenesis of the satellite lesions are unknown, although the intense concentration of periadnexal and perivascular nevus cells indicates that they could be caused by the infiltration and dissemination of nevus cells through the perivascular route.2,3
Clinical and Histologic Variants of Blue Nevus.
| Variant | Histologic Features |
|---|---|
| Common blue nevus | Dendritic melanocytes in the dermis |
| Cellular blue nevus | Dendritic melanocytes in the dermis admixed with cell islands (dumbbell pattern) |
| Combined blue nevus | Dendritic melanocytes in the dermis with abundant dendritic cells in the epidermis |
| Sclerosing blue nevus | Features of a blue nevus with exaggerated fibrosis in the dermis |
| Epithelioid blue nevus | Pigmented epithelioid melanocytes, few melanophages, and few dendritic melanocytes |
| Hypomelanotic/amelanotic blue nevus | Features of blue nevus with proliferation of cells associated with desmoplastic stroma |
| Plaque-type blue nevus | Features of common nevus with cellular nevus and infiltration of subcutaneous tissue |
| Deep penetrating blue nevus | Nevus cells extending into the dermis |
| Common blue nevus with satellite lesions | Features of common blue nevus |
| Agminated blue nevus | Features of common blue nevus |
| Atypical blue cellular nevus | Atypical cells with polymorphous nuclei |
| Malignant blue nevus | Malignant cells of melanocytic origin in the deep dermis with normal epidermal cells |
Source: Table modified from Savoia et al.7
Dermoscopic examination typically shows a diffuse homogeneous blue or steel blue structureless pattern, although polychromasia and structures typically associated with melanoma may be seen.6
Malignant transformation of blue nevus is a controversial topic,8–10 but there have been reports of the rare malignant blue nevus variant arising from a pre-existing blue nevus, at the site of an excised blue nevus, or in association with de novo melanoma. This clinical variant mainly affects patients like ours, i.e., men with lesions on the scalp.8,10
In conclusion, not all tumor lesions with satellite lesions are predictive of malignancy, but a histopathologic study is recommended because of the overlapping clinical and dermoscopic features.2,7,9,10
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Sardoy A, Bidabehere MB, Gubiani ML, Pinardi BA. Nevo azul con satelitosis que simula melanoma maligno. Actas Dermosifiliogr. 2018;109:377–378.



