

The aim of this study based on the records of the dermatology department of a tertiary referral hospital was to describe patients treated for allergic contact dermatitis induced by nickel between 2000 and 2010.
Materials and methodsFrom records of the skin allergy section of the dermatology department we extracted and analyzed information for patients who underwent patch testing with the standard series of the Spanish Contact Dermatitis Research Group (GEIDAC), which includes a patch with 5% nickel sulfate in petroleum jelly. The possibility that nickel release from various objects might have triggered the patient's dermatitis was assessed with the dimethylglyoxime spot test, which reveals a reddish precipitate if the metal is present.
ResultsA total of 3,404 patients underwent GEIDAC patch testing during the study period; 24.2% had positive reactions to the patch containing 5% nickel sulfate in petroleum jelly. However, the contact dermatitis could be attributed to nickel in only 57 of the 824 patients (6.9%) who showed sensitization to nickel.
ConclusionsPatch-test evidence of sensitization was found to be clinically relevant in only a small percentage of patients. We emphasize the usefulness of the dimethylglyoxime test to help establish the relevance of a positive nickel patch test. This test is even useful for identifying the specific object responsible for a patient's dermatitis.
El objetivo de este trabajo es el estudio descriptivo de los pacientes con dermatitis alérgica de contacto por níquel que han sido atendidos en un hospital de referencia en dermatología en un periodo de 10 años.
Material y métodosSe han analizado los datos de todos los pacientes parchados con la batería estándar del Grupo Español de Investigación en Dermatitis de Contacto y Alérgica Cutánea (GEIDAC) que incluye un parche con sulfato de níquel en vaselina al 5%, a partir de la base de datos informatizada de la sección de alergia cutánea de nuestro servicio. Para conocer la implicación de diferentes objetos metálicos en el origen de la dermatitis utilizamos un método colorimétrico llamado test de dimetilglioxima (DMGO).
ResultadosDurante el periodo de estudio se ha explorado mediante pruebas epicutáneas con la batería estándar del GEIDAC a 3.404 pacientes. Del total de pacientes parchados un 24,2% presentaron un parche positivo para sulfato de níquel al 5% en vaselina. Sin embargo, de los 824 pacientes sensibilizados al níquel solo en 57 de ellos (6,9%) se pudo demostrar una asociación de la sensibilización con la dermatitis por la que consultaban.
ConclusionesSolo se identificó relevancia presente en un pequeño porcentaje de pacientes con positividad al níquel en las pruebas epicutáneas. Destacamos la utilidad del test de DMGO como método de ayuda para establecer la relevancia de la positividad del parche con níquel, e incluso para conocer el objeto causante de dicha dermatitis.
Numerous epidemiologic studies on contact dermatitis show that sensitization to nickel is highly prevalent in Europe.1–3 Since this information is usually retrieved from data on patients with skin complaints who have been referred for patch testing, it does not generally apply to patients who consult directly for nickel-induced contact dermatitis, even if they are sensitized to nickel.
It is important to differentiate between prevalence of sensitization and prevalence of allergic contact dermatitis; hence the key role of relevance in positive patch test results.
In the case of nickel-induced allergic contact dermatitis, a colorimetric approach—the dimethylglyoxime spot test—can be used to determine the involvement of various metal objects in a skin disease. Not all objects that contain nickel necessarily release nickel. Those that do can be rapidly indentified using this simple test, which demonstrates the reaction between nickel and dimethylglyoxime by the formation of a reddish-brown precipitate.
Systematic implementation of this test would prove extremely useful when attempting to determine the cause of a skin disease and even for ascertaining which objects are causing contact dermatitis.
We performed a descriptive, observational, and retrospective study to evaluate nickel-induced contact dermatitis as the main presenting complaint in the skin allergy section of the dermatology department.
Material and MethodsStudy PopulationBetween January 2000 and December 2010, a total of 3404 patients underwent patch testing with the standard series of the Spanish Contact Dermatitis Research Group (GEIDAC), which includes a patch with 5% nickel sulfate in petroleum jelly. Data were obtained from the computerized database of the Skin Allergy Section of the Dermatology Department of Hospital Universitario de Valencia, Valencia, Spain. Readings were taken at 48 and 96hours using the evaluation criteria established by the International Contact Dermatitis Research Group (+, ++, +++).
Assessment of RelevanceRelevance was always assessed by the same researcher (Dr de la Cuadra), who classified the relevance of the patch test to nickel as follows: positive and present when sensitization was totally or partially associated with the clinical symptoms that led the patient to consult; and past when the patient remembered previous symptoms associated with sensitization (eg, dermatitis caused by objects such as earrings and watch strap fastenings). When none of the previous criteria were fulfilled, relevance was classed as negative or unknown.
Patients who reported contact with metallic objects at the site of their dermatitis (eg, hands, wrists, thighs, and abdomen) brought the objects (belt buckles, trousers with metallic buttons, watches, bracelets, necklaces, earrings, scissors, key rings, telephones, and prostheses) for the dimethylglyoxime test (Fig. 1).

Present relevance was defined as definite, probable, or possible as follows:
- -
Definite: gradual resolution of the complaint and positive dimethylglyoxime test result (eg, buckles, bracelets, garment fastenings, and key rings).
- -
Probable: gradual resolution of the complaint and negative dimethylglyoxime test result (eg, surgical staples and metallic body piercings).
- -
Possible: only clinical improvement and positive dimethylglyoxime test result, albeit with nonpermanent (occasional) contact items (eg, coins, scissors, tweezers, scrubbing pads, and metal scourers).
In this study, we only collected data from patients who had positive patch test results to nickel with positive and present relevance when this relevance was certain or at least probable.
Dimethylglyoxime TestThe test was performed using a 1% dimethylglyoxime solution in ethanol and a 9.9% ammonium hydroxide solution, both of which have been supplied by Laboratorios Menarini since 2000.
First, we moistened the white cotton of a swab with both solutions and rubbed them for 30seconds against the metal object. The test result was positive if the cotton turned red. We defined relevance as definite only when we demonstrated the presence of nickel with the dimethylglyoxime test in the object(s) that came into contact with the skin at the site of the dermatitis and as probable when we observed a gradual resolution of the complaint once the patient had eliminated all contact with the suspect metals, even if the dimethylglyoxime test had been negative (eg, surgical staples and metal body piercings).
ResultsWe collected data from the patients examined using the GEIDAC standard series between 2000 and 2010 (1283 men [37.7%] and 2121 women [62.3%]). The mean age of the population was 48.3 years.
Of the 3404 patients, 2092 (61%) had at least 1 positive patch test result for an allergen included in the standard series; in 824 patients (24.2%), the positive result was with 5% nickel sulfate in petroleum jelly.
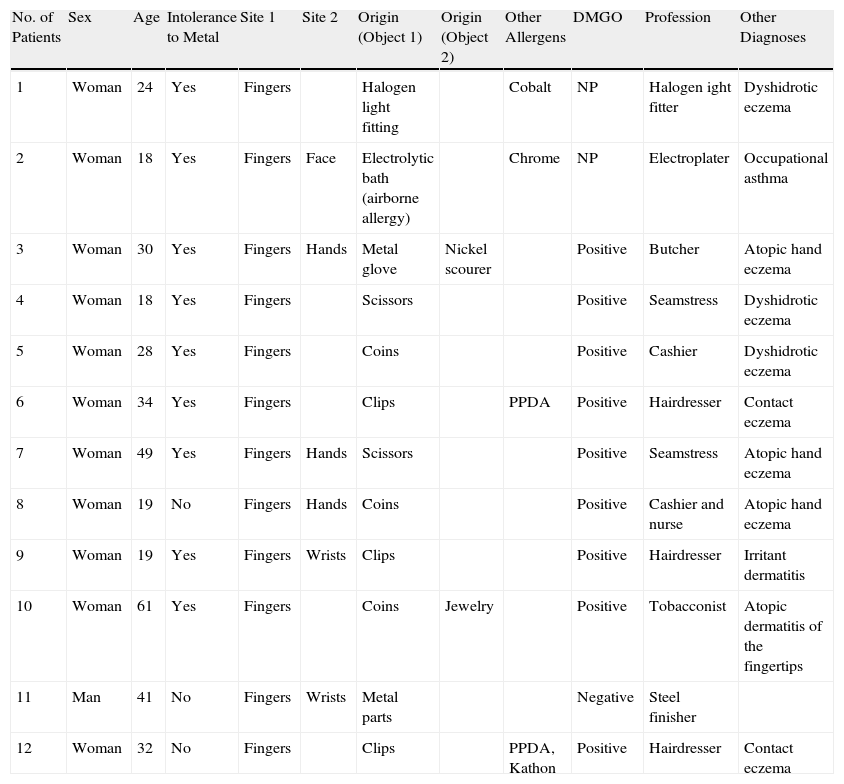
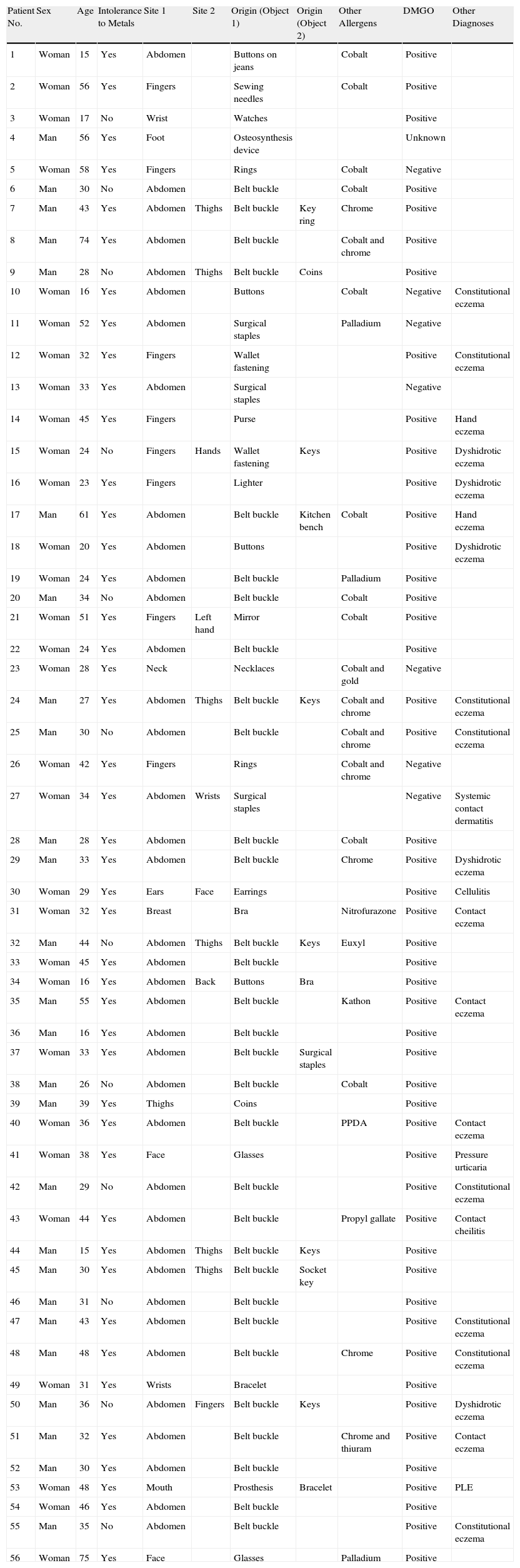
However, it is noteworthy that an association between sensitization and the presenting skin complaint was demonstrated in only 57 of the 824 nickel-sensitized patients (6.9%). The nickel allergy was considered occupational in 9 of the 57 patients (15.8%) (Table 1) and nonoccupational in 48 patients (84.2%) (Table 2).
Data for Patients With Occupational Allergic Contact Dermatitis in Hospital General Universitario de Valencia (2000-2010).
| No. of Patients | Sex | Age | Intolerance to Metal | Site 1 | Site 2 | Origin (Object 1) | Origin (Object 2) | Other Allergens | DMGO | Profession | Other Diagnoses |
| 1 | Woman | 24 | Yes | Fingers | Halogen light fitting | Cobalt | NP | Halogen ight fitter | Dyshidrotic eczema | ||
| 2 | Woman | 18 | Yes | Fingers | Face | Electrolytic bath (airborne allergy) | Chrome | NP | Electroplater | Occupational asthma | |
| 3 | Woman | 30 | Yes | Fingers | Hands | Metal glove | Nickel scourer | Positive | Butcher | Atopic hand eczema | |
| 4 | Woman | 18 | Yes | Fingers | Scissors | Positive | Seamstress | Dyshidrotic eczema | |||
| 5 | Woman | 28 | Yes | Fingers | Coins | Positive | Cashier | Dyshidrotic eczema | |||
| 6 | Woman | 34 | Yes | Fingers | Clips | PPDA | Positive | Hairdresser | Contact eczema | ||
| 7 | Woman | 49 | Yes | Fingers | Hands | Scissors | Positive | Seamstress | Atopic hand eczema | ||
| 8 | Woman | 19 | No | Fingers | Hands | Coins | Positive | Cashier and nurse | Atopic hand eczema | ||
| 9 | Woman | 19 | Yes | Fingers | Wrists | Clips | Positive | Hairdresser | Irritant dermatitis | ||
| 10 | Woman | 61 | Yes | Fingers | Coins | Jewelry | Positive | Tobacconist | Atopic dermatitis of the fingertips | ||
| 11 | Man | 41 | No | Fingers | Wrists | Metal parts | Negative | Steel finisher | |||
| 12 | Woman | 32 | No | Fingers | Clips | PPDA, Kathon | Positive | Hairdresser | Contact eczema |
Abbreviations: DMGO, dimethylglyoxime; NP, not performed; PPDA, paraphenylenediamine.
Data for Patients With Nonoccupational Allergic Contact Dermatitis at Hospital General Universitario de Valencia (2000-2010).
| Patient No. | Sex | Age | Intolerance to Metals | Site 1 | Site 2 | Origin (Object 1) | Origin (Object 2) | Other Allergens | DMGO | Other Diagnoses |
| 1 | Woman | 15 | Yes | Abdomen | Buttons on jeans | Cobalt | Positive | |||
| 2 | Woman | 56 | Yes | Fingers | Sewing needles | Cobalt | Positive | |||
| 3 | Woman | 17 | No | Wrist | Watches | Positive | ||||
| 4 | Man | 56 | Yes | Foot | Osteosynthesis device | Unknown | ||||
| 5 | Woman | 58 | Yes | Fingers | Rings | Cobalt | Negative | |||
| 6 | Man | 30 | No | Abdomen | Belt buckle | Cobalt | Positive | |||
| 7 | Man | 43 | Yes | Abdomen | Thighs | Belt buckle | Key ring | Chrome | Positive | |
| 8 | Man | 74 | Yes | Abdomen | Belt buckle | Cobalt and chrome | Positive | |||
| 9 | Man | 28 | No | Abdomen | Thighs | Belt buckle | Coins | Positive | ||
| 10 | Woman | 16 | Yes | Abdomen | Buttons | Cobalt | Negative | Constitutional eczema | ||
| 11 | Woman | 52 | Yes | Abdomen | Surgical staples | Palladium | Negative | |||
| 12 | Woman | 32 | Yes | Fingers | Wallet fastening | Positive | Constitutional eczema | |||
| 13 | Woman | 33 | Yes | Abdomen | Surgical staples | Negative | ||||
| 14 | Woman | 45 | Yes | Fingers | Purse | Positive | Hand eczema | |||
| 15 | Woman | 24 | No | Fingers | Hands | Wallet fastening | Keys | Positive | Dyshidrotic eczema | |
| 16 | Woman | 23 | Yes | Fingers | Lighter | Positive | Dyshidrotic eczema | |||
| 17 | Man | 61 | Yes | Abdomen | Belt buckle | Kitchen bench | Cobalt | Positive | Hand eczema | |
| 18 | Woman | 20 | Yes | Abdomen | Buttons | Positive | Dyshidrotic eczema | |||
| 19 | Woman | 24 | Yes | Abdomen | Belt buckle | Palladium | Positive | |||
| 20 | Man | 34 | No | Abdomen | Belt buckle | Cobalt | Positive | |||
| 21 | Woman | 51 | Yes | Fingers | Left hand | Mirror | Cobalt | Positive | ||
| 22 | Woman | 24 | Yes | Abdomen | Belt buckle | Positive | ||||
| 23 | Woman | 28 | Yes | Neck | Necklaces | Cobalt and gold | Negative | |||
| 24 | Man | 27 | Yes | Abdomen | Thighs | Belt buckle | Keys | Cobalt and chrome | Positive | Constitutional eczema |
| 25 | Man | 30 | No | Abdomen | Belt buckle | Cobalt and chrome | Positive | Constitutional eczema | ||
| 26 | Woman | 42 | Yes | Fingers | Rings | Cobalt and chrome | Negative | |||
| 27 | Woman | 34 | Yes | Abdomen | Wrists | Surgical staples | Negative | Systemic contact dermatitis | ||
| 28 | Man | 28 | Yes | Abdomen | Belt buckle | Cobalt | Positive | |||
| 29 | Man | 33 | Yes | Abdomen | Belt buckle | Chrome | Positive | Dyshidrotic eczema | ||
| 30 | Woman | 29 | Yes | Ears | Face | Earrings | Positive | Cellulitis | ||
| 31 | Woman | 32 | Yes | Breast | Bra | Nitrofurazone | Positive | Contact eczema | ||
| 32 | Man | 44 | No | Abdomen | Thighs | Belt buckle | Keys | Euxyl | Positive | |
| 33 | Woman | 45 | Yes | Abdomen | Belt buckle | Positive | ||||
| 34 | Woman | 16 | Yes | Abdomen | Back | Buttons | Bra | Positive | ||
| 35 | Man | 55 | Yes | Abdomen | Belt buckle | Kathon | Positive | Contact eczema | ||
| 36 | Man | 16 | Yes | Abdomen | Belt buckle | Positive | ||||
| 37 | Woman | 33 | Yes | Abdomen | Belt buckle | Surgical staples | Positive | |||
| 38 | Man | 26 | No | Abdomen | Belt buckle | Cobalt | Positive | |||
| 39 | Man | 39 | Yes | Thighs | Coins | Positive | ||||
| 40 | Woman | 36 | Yes | Abdomen | Belt buckle | PPDA | Positive | Contact eczema | ||
| 41 | Woman | 38 | Yes | Face | Glasses | Positive | Pressure urticaria | |||
| 42 | Man | 29 | No | Abdomen | Belt buckle | Positive | Constitutional eczema | |||
| 43 | Woman | 44 | Yes | Abdomen | Belt buckle | Propyl gallate | Positive | Contact cheilitis | ||
| 44 | Man | 15 | Yes | Abdomen | Thighs | Belt buckle | Keys | Positive | ||
| 45 | Man | 30 | Yes | Abdomen | Thighs | Belt buckle | Socket key | Positive | ||
| 46 | Man | 31 | No | Abdomen | Belt buckle | Positive | ||||
| 47 | Man | 43 | Yes | Abdomen | Belt buckle | Positive | Constitutional eczema | |||
| 48 | Man | 48 | Yes | Abdomen | Belt buckle | Chrome | Positive | Constitutional eczema | ||
| 49 | Woman | 31 | Yes | Wrists | Bracelet | Positive | ||||
| 50 | Man | 36 | No | Abdomen | Fingers | Belt buckle | Keys | Positive | Dyshidrotic eczema | |
| 51 | Man | 32 | Yes | Abdomen | Belt buckle | Chrome and thiuram | Positive | Contact eczema | ||
| 52 | Man | 30 | Yes | Abdomen | Belt buckle | Positive | ||||
| 53 | Woman | 48 | Yes | Mouth | Prosthesis | Bracelet | Positive | PLE | ||
| 54 | Woman | 46 | Yes | Abdomen | Belt buckle | Positive | ||||
| 55 | Man | 35 | No | Abdomen | Belt buckle | Positive | Constitutional eczema | |||
| 56 | Woman | 75 | Yes | Face | Glasses | Palladium | Positive |
Abbreviations: DMGO, dimethylglyoxime; PLE, polymorphous light eruption.
Both tables show clinical data from patients with positive patch test results with present and definite relevance (positive dimethylglyoxime test result) and probable relevance (negative dimethylglyoxime test result). The dimethylglyoxime test made it possible to investigate the release of nickel from the metal objects brought by the patients in 65 of 68 cases. The test result was positive in 57 cases and negative in 8 cases.
In other words, of the 824 patients who were sensitized to nickel, the presenting skin complaint was shown to be induced by nickel in the objects handled in 57 cases; in the remaining 8 cases, sensitization to nickel was probably associated with the presenting skin complaint, that is, the dimethylglyoxime test result was negative, but the skin complaint resolved when the patient stopped using the causative object.
In the 57 cases of nonoccupational allergic contact dermatitis of present relevance, the association between dermatitis and the use of various objects and garments was demonstrated, and the site of the dermatitis coincided with the area of contact with the metal objects (eg, buckle with abdomen and key ring with thigh).
Many of the patients with nickel-induced allergic contact dermatitis simultaneously presented other skin complaints, and even systemic manifestations not associated with allergy to metal (dyshidrotic eczema [8 cases], constitutional eczema [8 cases], contact eczema caused by other allergens [7 cases], atopic dermatitis [4 cases], polymorphic light eruption [1 case], occupational asthma [1 case], and pressure urticaria [1 case]).
DiscussionEvaluation of the relevance of a positive result is the most difficult part of the patch test procedure. It depends on the skill, experience, and curiosity of the researcher, and, particularly in a case of past relevance, on the patient's memory.
The first data on sensitization to nickel in Spain were reported in 19764; however, the clinical relevance of this sensitization was not included in the epidemiologic studies of the GEIDAC until 1996,5 when, of the 3386 patients examined, 993 (29.3%) were sensitized to nickel; of these, 37% had present and positive relevance, ie, they consulted for allergic dermatitis caused by contact with nickel.
A subsequent study by GEIDAC in the year 20016 showed similar percentages of sensitization (26.64%) and of present positive relevance (36.38%).
In the year 2008, the Spanish Surveillance System on Contact Allergies (REVAC)7 reported that the frequency of sensitization to nickel was 25.4%. Relevance was present in 32% of the 295 patients sensitized to nickel.
Over a period of 10 years (2000-2010), we found a very similar percentage (24.2%) in 3404 patients. However, we only found present relevance in 6.9% of the 824 positive cases. We believe that this difference is due to the subjectivity involved in determination of present relevance, which may be definite (dimethylglyoxime test), probable (clearly observable clinical course), or only possible (eg, frequent contact with coins in hand eczema).8 We only included patients with definite present relevance. In other studies, it is possible that relevance was considered present when it was only probable or possible. This observation could explain the disparate percentages for positive and present relevance (7.89% vs 36.38% and 32%). It is also noteworthy that, for patients whose sensitization was of present relevance, none of the previous studies6,7,9 established the site, specific origin, or cause of the eczema, as we did.
Similarly, Spanish epidemiologic studies do not state that authors use the dimethylglyoxime test routinely in their clinical practice. In our opinion, the fact that a patient has come into contact with a metal object (eg, stainless steel, which is a nickel-containing alloy) does not mean that this object caused his/her dermatitis. Alloys with high nickel content do not always release nickel, or if they do, they do so in amounts of less than 5mg/cm2/wk, which is the minimum quantity for triggering dermatitis in a patient who was previously sensitized to this metal.10
The dimethylglyoxime test has a specificity of 97.5%, although its sensitivity is only 59.3%.11
In summary, we performed an observational and retrospective study by collecting data on patients sensitized to nickel in our hospital from January 2000 to December 2010 in order to ascertain which of these patients genuinely had allergic contact dermatitis due to this metal and how many consulted for this reason. We emphasize the usefulness of the dimethylglyoxime test when attempting to establish the relevance of a positive nickel patch test result. The test could even prove useful to identify the object responsible for the patient's dermatitis.
Ethical DisclosuresProtection of persons and animalsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed their hospital's protocol on the publication of data concerning patients and that all patients included in the study have received sufficient information and have given their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: García-Rabasco AE, Zaragozá-Ninet V, García-Ruíz R, de la Cuadra-Oyanguren J. Dermatitis alérgica de contacto a níquel. Estudio descriptivo en un hospital terciario en la década del 2000 al 2010. Actas Dermosifiliogr. 2014;105:590–596.


