



A 57-year-old male farmer with no relevant personal or family medical history and no known diseases presented with a lesion on the inner aspect of the left leg that had appeared about 10 years previously. The lesion was asymptomatic, had never bled, and had slowly and progressively grown over the years.
Physical ExaminationPhysical examination revealed an exophytic, polypoid tumor with a broad base and no adhesion to the deeper layers. The tumor was soft with a friable, erythematous, fleshy surface and measured 3cm in diameter (Fig. 1).

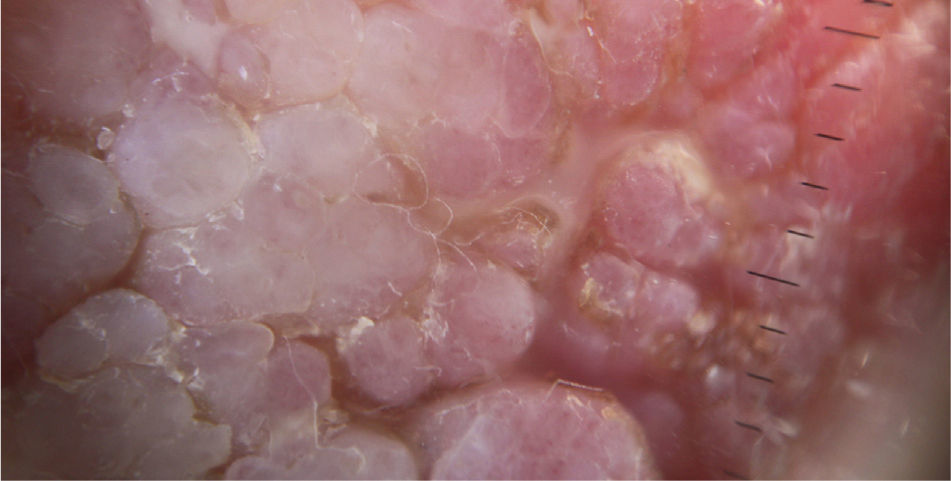
Dermoscopy revealed that the tumor surface consisted of multiple raised structures interconnected in a honeycomb pattern and displayed some whitish radial streaks and fine arborizing telangiectasias (Fig. 2).
Locoregional lymph nodes were not palpable and no other significant abnormalities were observed in the physical examination.
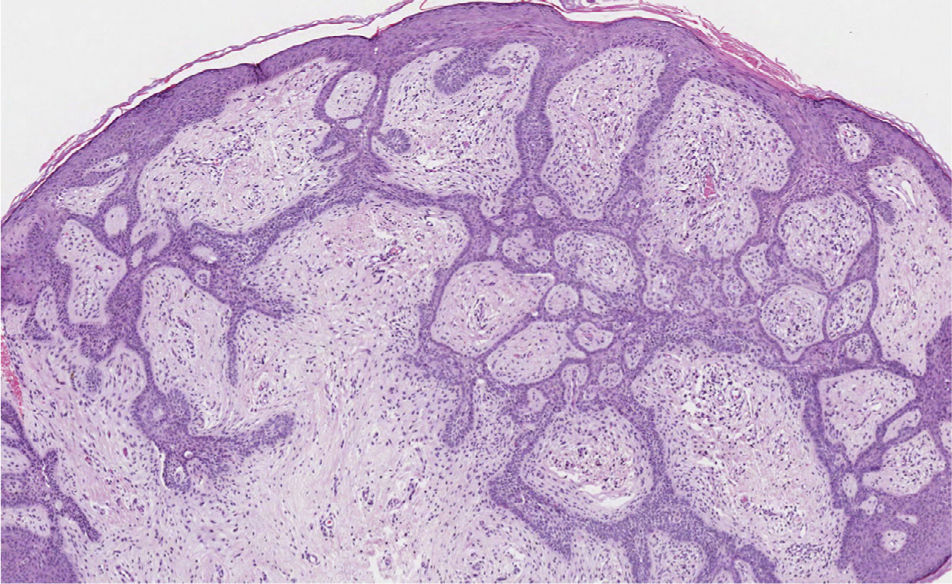
HistopathologyHistopathology with hematoxylin-eosin (original magnification ×20) revealed a tumor composed of thin, elongated, anastamosing strands of basaloid cells that were connected to the epidermis and extended down towards the dermis forming a lattice-like pattern within a dense fibrotic stroma (Fig. 3).
What Is Your Diagnosis?
DiagnosisFibroepithelioma of Pinkus.
Clinial Course and TreatmentUnder local anesthesia, the patient underwent surgical excision with margins and direct closure, without complications. After 6 months of follow-up the patient has a nonpathological scar with no signs of local recurrence or new lesions.
CommentFibroepithelioma of Pinkus, initially described in 1953 as a premalignant fibroepithelial tumor of the skin,1 is a benign neoplasm with differentiation toward follicular germinative cells. This tumor has been traditionally considered a rare variant of basal cell carcinoma (BCC), based on its characteristic histopathological features. Histologically, the tumor consists of strands of interconnected basaloid epithelia coated with preexisting follicular infundibula that connect to the epidermis to form a fenestrated pattern, with occasional solid islands of basaloid cells, a dense fibrotic stroma, and a rich capillary network.2 In some cases the cytology, stroma, and architectural features suggest that this tumor type would be more correctly classified as a retiform variant of trichoblastoma rather than a BCC.3 However, it does not display as advanced a degree of follicular differentiation as seen in trichoblastoma.
Fibroepithelioma of Pinkus affects men and women similarly, and appears in individuals between 40 and 60 years of age. The most common location is the trunk. It has a predilection for unexposed areas (unlike BCC), especially the lumbosacral area, although it can develop in any anatomic site except areas of skin that lack hair follicles. While the tumor manifests clinically as an initially flat lesion, it grows progressively and causes few symptoms, and can thus reach a large size, as seen in our patient. It is scarcely aggressive and has a good prognosis; no distant metastases have been described.
The dermoscopic pattern of this tumor has been described; the key features are arborized telangiectasias that are longer and finer than those seen in BCC and whitish streaks caused by abundant fibrovascular stroma. These correspond respectively to the brownish maple leaf and spoke-wheel structures seen in classic BCC.4
The differential diagnosis of Fibroepithelioma of Pinkus includes squamous cell carcinoma, amelanotic melanoma, skin metastasis, Merkel cell carcinoma, and primary cutaneous diffuse large B-cell lymphoma, leg type. However, those tumors are malignant skin neoplasms characterized by rapid growth and a poor prognosis, features that are not concordant with the clinical course of our patient's tumor. Therefore, the differential diagnosis must also include other less common benign neoplasms with follicular differentiation in which the definitive diagnosis is established by histopathology; these include large solitary trichodiscoma, trichoadenoma, fibroadenoma, and eccrine syringofibroadenoma, as well as other tumors such as lymphoepithelial tumor of the skin.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: López-Villaescusa MT, de Manueles Marcos F, Pérez García LJ. Lesión pediculada de crecimiento lento. Actas Dermosifiliogr. 2014;105:789–790.



