






Female androgenetic alopecia (FAA) has considerable impact on quality of life. Our analysis of the clinical scales available in the literature to measure the impact of FAA led us to choose the Hair Specific Skindex 29 (HSS29) as the most appropriate for adaptation to Spanish as a tool for following patients in treatment for FAA. This tool assesses disease impact on quality of life over time so that treatments can be tailored to patients’ needs. The HSS29 score reflects impact in 3 domains (emotions, symptoms, and functioning) on a scale of 0 (no effect) to 100 (maximum effect). The scale is useful in routine clinical practice, and patients can respond to all items in 5minutes.
Materials and methodsWe followed recommended procedures to produce a cross-cultural adaptation of the scale. The process involved forward translation of the questionnaire to Spanish followed by back translation by 2 native speakers of the original language (English) and revision as needed after discussion and consensus by a committee of 3 expert dermatologists. The comprehensibility of the resulting translation was assessed in a test–retest step. Next, the psychometric properties, reliability, and construct validity were assessed. Sensitivity and specificity were evaluated with the area under the receiver operating characteristic (ROC) curve, reliability with Cronbach's α, and construct validity by factor analysis using a Varimax rotation. Face validity was also assessed during the process. The intraclass correlation coefficient (ICC) was calculated in the test–retest step.
ResultsA total of 170 women with FAA and 30 control subjects completed the cross-culturally adapted Spanish questionnaire. A subgroup of 15 subjects responded a second time between 1 and 2 days after their first session (test–retest). Sensitivity and specificity were excellent according to the area under the ROC curve (0.98; 95% CI, 0.97–0.99), and high reliability was reflected by a Cronbach's α of 0.96. Factor analysis showed that the items were grouped in the same 3 domains (functioning, emotions, and symptoms) as in the original version of the scale. There were no significant differences in the mean (SD) scores on the test and the retest (23.05 [16.42] vs 22.01 [17.72], respectively). The ICC of over 0.9 indicated excellent correlation between responses to the adapted Spanish version.
ConclusionsThe psychometric properties of the Spanish version of the HSS29 are similar to those of the original scale. The Spanish HSS29 is a useful tool for assessing quality of life in FAA.
La alopecia femenina tiene un impacto importante sobre la calidad de vida. Analizadas las escalas publicadas para medir este impacto, hemos considerado que la escala Hair Specific Skindex 29 (HSS29) es la más adecuada para el objetivo del proyecto: obtener una herramienta en español para el seguimiento en el tratamiento de la alopecia androgenética femenina, que permita medir la evolución del impacto en la calidad de vida y adaptar e individualizar el tratamiento a las necesidades de la mujer. La escala HSS29 puntúa entre 0 (nula afectación) y 100 (total afectación) y discrimina 3dominios (emociones, síntomas y función), siendo una escala útil en la práctica clínica diaria, autocumplimentada en menos de 5 min.
Materiales y métodosSe realizó el proceso metodológico establecido para la validación transcultural de una escala, a través de la traducción y retrotraducción por 2traductores nativos en la lengua original de la escala (inglés), con el consenso de un comité de 3dermatólogos expertos cuando fuera necesario. La versión consensuada se sometió a un pretest con pacientes para comprobar la correcta comprensión. Posteriormente, se determinaron las características psicométricas de la escala, la fiabilidad y su validez de constructo (sensibilidad y especificidad mediante curva ROC, fiabilidad por alfa de Cronbach, constructo por análisis factorial con rotación Varimax), de apariencia y la validez test-retest (correlación intraclase).
ResultadosCiento setenta mujeres con alopecia y 30 controles respondieron a la escala. Un subgrupo de 15 pacientes realizó el test-retest y respondieron a la escala tras 1-2 días de la valoración inicial. La escala presentó una excelente sensibilidad y especificidad medida por la curva ROC 0,98 (intervalo de confianza del 95%, 0,97-0,99) y una muy elevada fiabilidad con alfa de Cronbach de 0,96. El análisis factorial mostró que los ítems se distribuyeron en las 3dimensiones (funcional, emociones y síntomas) como en la escala original. No se encontraron diferencias significativas entre los valores del test y del retest (23,05 ± 16,42 vs 22,01 ± 17,72, p = ns) y el coeficiente de correlación intraclase fue excelente (superior a 0,9).
ConclusionesLa versión española de la escala HSS29 presenta unas características psicométricas similares a la escala original y es una herramienta útil para la evaluación de la calidad de vida en alopecia femenina.

Alopecia accounts for 3%-8% of all first visits to dermatology clinics. Female androgenetic alopecia is the most important form of hair loss owing to its high frequency, significant emotional repercussions, and effect on quality of life.1 The impact of alopecia is greater in women than in men, with 52% of women reporting being very concerned about hair loss, compared with 28% of men.2 Even slight hair loss has been associated with diminished quality of life.3,4 The incidence of female androgenetic alopecia peaks at 2points in a woman's life: at 30 years and at 50-60 years. Overall, approximately 50% of men and 40% of women are affected by androgenetic alopecia when they reach age 50 years.5,6
Knowing how female androgenetic alopecia affects health-related quality of life (HRQOL) could enable us to tailor treatment. The Skindex-29 Scale was developed by Chren et al.7 to evaluate quality of life in patients with specific skin problems. The scale covers 29 items in the field of dermatology and can be completed by the patient in 5minutes. It has been validated in the United States of America and shown to be internally consistent (Cronbach α, 0.87-0.96) and reproducible (r = 0.88-0.92) and have content and construct validity.7 Han et al.8 subsequently modified the scale to evaluate HRQOL specifically in patients with alopecia, thus leading to the development of the Hair Specific Skindex-29 Scale. However, this scale is available in English. A Spanish-language version of the scale could enable more integrated management of female androgenetic alopecia in Spain. The objective of the present study was to evaluate the comprehension of the items comprising the original Hair Specific Skindex-29 Scale and perform a cross-cultural validation to Spanish.
Materials and MethodsStudy DesignThe study was carried out between January and April 2017, after approval by the Ethics Committee of Hospital Universitario 12 de Octubre, Madrid, Spain. In the first phase, the Hair Specific Skindex-29 questionnaire was cross-culturally adapted and translated into Spanish following the 5 stages set out in the international literature9,10: (1) forward translation of the original questionnaire to Spanish by at least 2bilingual translators independently; (2) synthesis of the translations and resolution of possible discrepancies; (3) back translation of the consensus version in Spanish to the original by at least 2independent translators who were not familiar with the original version of the scale; (4) review by an expert committee to ensure semantic, linguistic, and conceptual equivalence; and (5) pilot testing to determine how well the translated questionnaire is understood by a group of women similar to those of the target population. This phase finished with a final version of the Hair-Specific Skindex-29 that was ready for validation.
In the second phase, the questionnaire that had been cross-culturally adapted and translated into Spanish was validated. We evaluated the face validity, reliability (Cronbach α), construct validity (factor analysis with Varimax rotation), and test–retest validity. Similarly, we evaluated the sensitivity, specificity, and internal consistency to determine discriminative power. A panel of dermatologists from 10Spanish autonomous communities participated in the validation process. Face validity makes it possible to ensure that the questionnaire measures what it is supposed to measure in a logical way and find differences between patients and healthy participants. This was done by providing the Hair-Specific Skindex-29 questionnaire to a selection of women with alopecia (cases) and a group of healthy women (controls) and instructing them on the need to respond to the questionnaire themselves. The content and construct validity makes it possible to ensure that the Spanish version measures the same aspects as the original scale, both in terms of the items and in terms of the domain structure. Test–retest validity was assessed to ensure the reproducibility and reliability of the questionnaire, that is, its optimal functioning under various conditions. Therefore, 5 patients with alopecia included by 3 different investigators were asked to complete the Hair Specific Skindex-29 questionnaire on 2occasions separated by 1-2 days. For the global evaluation of the scale in clinical practice, it was proposed to consider a score of ≥ 20 points mild involvement, a score of ≥ 30 points moderate involvement, and a score of ≥ 40 points severe involvement.
PatientsThe pilot comprehensibility test (pretest) was performed with the translated and cross-culturally adapted self-administered Hair Specific Skindex-29 in a sample of Spanish-speaking women aged ≥18 years with and without alopecia. Health professionals were excluded from the pretest. The process of cross-cultural validation to the Spanish language was carried out in women aged ≥18 years who visited 17 dermatology clinics throughout Spain. The selection comprised a sample of women with various grades of alopecia (cases) according to the scale of Dinh and Sinclair2 and a sample of women without alopecia (controls). The analysis of reliability and construct requires at least 5 cases for each item on the instrument, although not fewer than 100 patients in total.11 Since the scale has 29 items, at least 145 cases are necessary.
Hair-Specific Skindex-29 QuestionnaireHair Specific Skindex-29 is a self-administered instrument that makes it possible to evaluate HRQOL in patients with alopecia. It was developed from the Skindex-29 scale and comprises 29 items distributed into 3 dimensions or domains: the symptom domain (7 items), the function domain (12 items), and the emotion domain (10 items). Mean time for completion is 5minutes, and each item has a response scale comprising 5 response options ranging from 0 (never) to 5 (all the time). The score for each domain is obtained by converting the sum of all the responses into a linear scale ranging from 0 (no effect on HRQOL) to 100 (maximum effect on HRQOL).
Statistical analysisData were analyzed using SAS, Version 9.4 (SAS Institute Inc.). The discriminative power of the questionnaire was demonstrated using a receiver operating characteristic (ROC) curve based on logistic regression. The questionnaire was considered not to be discriminative if the ROC curve coincided with the line of no discrimination, which has an area under the curve (AUC) of 0.50. The discriminative power of the questionnaire increases as the AUC approaches 1.00.12 The sensitivity and specificity of the questionnaire were evaluated using the Youden index,13 which attempts to identify the cutoff in the questionnaire score that optimizes the relationship between sensitivity and specificity for detecting cases. The Cronbach α was used to estimate the reliability of the questionnaire.14 Measurement of reliability using the Cronbach α assumes that the items assess the same construct and that they are highly correlated. Following the criterion of George and Mallery,15 a Cronbach α ≥ 0.90 indicates excellent reliability. The Cronbach α was also calculated after elimination of some items to ensure that the items were homogeneous and that the scale consistently measured the characteristic for which it was designed if any questions were eliminated. Construct validity was analyzed using exploratory factor analysis with a Varimax rotation to determine whether the items on the questionnaire were associated with the 3domains (function, symptom, and emotion) in the same way as the original questionnaire.16 Test–retest reliability was assessed using the method proposed by Bland and Altman17–19 and the intraclass correlation coefficient proposed by Shrout and Fless (1979).20 An intraclass correlation coefficient >0.90 indicates high reliability for the questionnaire.21
ResultsA total of 17 women (mean age, 38.4 years) took the test to determine the comprehensibility of the translated questionnaire (Table 1); the level of comprehensibility recorded was appropriate. Thirty percent of the women had alopecia of varying intensity. In order to perform the cross-cultural validation to Spanish, the Hair Specific Skindex-29 was administered to 170 women (mean [SD] age, 47.54 [17.10] years; 95% CI, 44.95-50.12) with alopecia of different grades (cases) according to the Sinclair scale. The most common grade was grade ii, which affected 43.53%. The questionnaire was also administered to 30healthy women (controls) (mean age, 41.47 [12.67] years [95% CI, 36.71-46.23]). All of the questionnaires (100%) received were analyzed. Table 2 shows the different grades of alopecia in the cases. No statistically significant differences were observed between the cases and controls with respect to age or educational level.
Items on the Hair Specific Skindex-29 Scale.
| 1. My scalp hurts |
| 2. My alopecia affects how well I sleep |
| 3. I worry that my alopecia may be serious |
| 4. My alopecia makes it hard to work or do hobbies |
| 5. My alopecia affects my social life |
| 6. My alopecia makes me feel depressed |
| 7. My scalp burns or stings |
| 8. I tend to stay at home because of my alopecia |
| 9. I worry about getting scars because of my alopecia |
| 10. My scalp itches |
| 11. My alopecia affects how close I can be with those I love |
| 12. I am ashamed of my alopecia |
| 13. I worry that my alopecia may get worse |
| 14. I tend to do things by myself because of my alopecia |
| 15. I am angry about my alopecia |
| 16. Water bothers my scalp (bathing, washing hands) |
| 17. My alopecia makes showing affection difficult |
| 18. My scalp is irritated |
| 19. My alopecia affects my interactions with others |
| 20. I am embarrassed by my alopecia |
| 21. My alopecia is a problem for the people I love |
| 22. I am frustrated by my alopecia |
| 23. My scalp is sensitive |
| 24. My alopecia affects my desire to be with people |
| 25. I am humiliated by my alopecia |
| 26. My scalp bleeds |
| 27. I am annoyed by my alopecia |
| 28. My alopecia interferes with my sex life |
| 29. My alopecia makes me tired |
This table is an English translation of the Spanish version of the items comprising the Hair Specific Skindex-29.
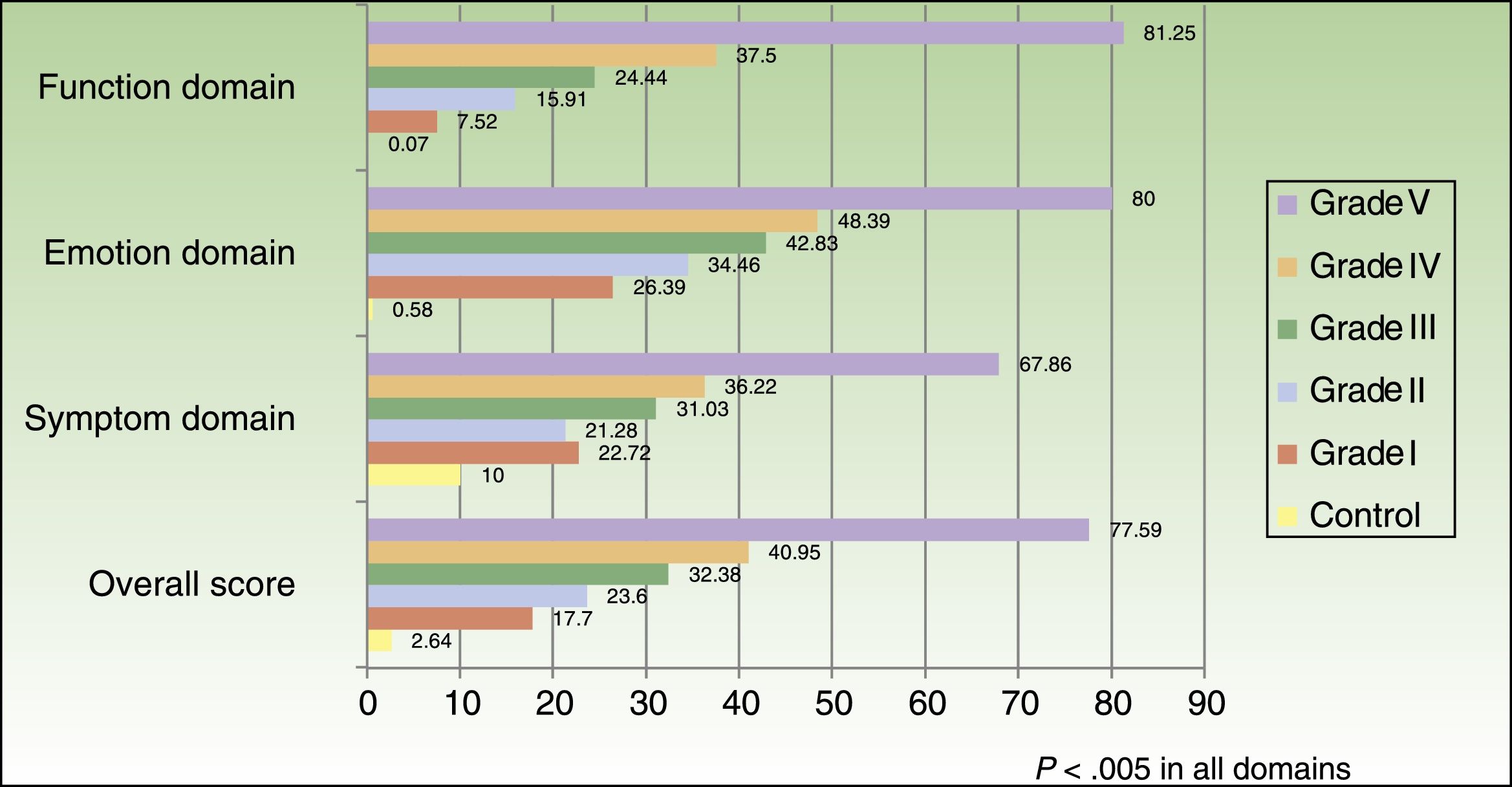
Statistically significant differences were observed between cases and controls with respect to the overall score in the Hair Specific Skindex-29 questionnaire and in the 3domains (function, emotion, and symptom) (P < .005). Table 3 shows that scores were significantly higher for women with alopecia than for healthy women in the cross-culturally adapted Spanish version of Hair Specific Skindex-29. For women with alopecia, the highest score was obtained in the emotion domain. Similarly, we observed that the score increased with the grade of alopecia and that the highest impact was observed in the emotion domain. This impact was already evident at Sinclair grade i alopecia (Fig. 1).
Difference in Scores Between Cases and Controls in the Spanish Version of the Hair Specific Skindex-29 Questionnaire.
| Score, mean (SD)a | ||||
|---|---|---|---|---|
| Global | Function Domain | Emotion Domain | Symptom Domain | |
| Controls (n = 30) | 2.64 (3.86) | 0.07 (0.38) | 0.58 (2.24) | 10 (15.62) |
| Cases (n = 170) | 26.42 (18.90) | 18.55 (21.13) | 36.38 (23.97) | 25.67 (19.65) |
When the results were stratified by age group, the highest score was observed for women with alopecia aged < 45 years, both overall and in each of the domains (P < .005). Table 4 shows the results by age group (cases only). No differences were observed in the overall scores on the questionnaire with respect to educational level.
Results for the Score on the Hair Specific Skindex-29 Questionnaire by Age Group (Cases Only).
| Score, Mean (SD) | ||||
|---|---|---|---|---|
| Global | Function Domain | Emotion Domain | Symptom Domain | |
| 0-44 y (n = 77) | 33.61 (21.53) | 26.46 (25.07) | 43.93 (25.82) | 31.12 (20.06) |
| 45-65 y (n = 59) | 21.27 (12.99) | 12.29 (13.48) | 32.25 (20.58) | 21.00 (17.62) |
| > 65 y (n = 34) | 19.07 (15.57) | 11.52 (15.88) | 26.47 (19.97) | 21.43 (19.44) |
| Total cases (N = 170) | 26.42 (18.90) | 18.55 (21.13) | 36.38 (23.97) | 25.67 (19.65) |
The Cronbach α based on the total number of questionnaires was 0.96, thus indicating that the internal reliability was excellent. When each of the items on the questionnaire was eliminated individually, the Cronbach α did not improve, indicating that no item can be eliminated. The power of the questionnaire to discriminate between cases measured using the ROC curve made it possible to obtain an AUC of 0.95 (95% CI, 0.92-0.98), considering values > 0.9 as very good. The evaluation of sensitivity and specificity using the Youden index made it possible to obtain a cutoff in the Hair Specific Skindex-29 greater than 6.034. This cutoff gave the questionnaire a very high sensitivity, 0.93, and a specificity for detecting cases of 0.9 and would generate 158 true positives (93%), 27 true negatives, 3 false positives, and 12 false negatives (7.05%).
In the exploratory factor analysis of the responses to the questionnaire items performed to examine the factor structure of the scores and identify the underlying domain (number of factors with an eigenvalue > 1), 3 domains with a value > 1 are selected, as in the original Hair Specific Skindex-29.
The Varimax-rotated components matrix for 3 factors plays a role in validating the construct of the scale, showing that the items tend to group together in the domains (function, emotion, and symptom) proposed in the original scale (Table 5).
Matrix of Varimax-Rotated Components in the Factor Model of the Hair Specific Skindex-29 (Cases Only).
| Rotated Factor Model | ||||
|---|---|---|---|---|
| Item | Function Domain | Emotion Domain | Symptom Domain | |
| Item 02 | My alopecia affects how well I sleep | 0.41 | ||
| Item 05 | My alopecia affects my social life | 0.53 | 0.59 | |
| Item 29 | My alopecia makes me tired | 0.57 | ||
| Item 04 | My alopecia make it hard to work or do hobbies | 0.61 | ||
| Item 21 | My alopecia is a problem for the people I love | 0.62 | ||
| Item 17 | My alopecia makes showing affection difficult | 0.72 | ||
| Item 11 | My alopecia affects how close I can be with those I love | 0.73 | ||
| Item 19 | My alopecia affects my interactions with others | 0.76 | ||
| Item 24 | My alopecia affects my desire to be with people | 0.78 | ||
| Item 08 | I tend to stay at home because of my alopecia | 0.78 | ||
| Item 14 | I tend to do things by myself because of my alopecia | 0.79 | ||
| Item 28 | My alopecia interferes with my sex life | 0.80 | ||
| Item 09 | I worry about getting scars because of my alopecia | 0.40 | 0.30 | 0.35 |
| Item 03 | I worry that my alopecia may be serious | 0.45 | ||
| Item 20 | I am embarrassed by my alopecia | 0.60 | 0.57 | |
| Item 13 | I worry that my alopecia may get worse | 0.66 | ||
| Item 25 | I am humiliated by my alopecia | 0.66 | ||
| Item 15 | I am angry about my alopecia | 0.73 | ||
| Item 22 | I am frustrated by my alopecia | 0.74 | ||
| Item 12 | I am ashamed of my alopecia | 0.75 | ||
| Item 06 | My alopecia makes me feel depressed | 0.76 | ||
| Item 27 | I am annoyed by my alopecia | 0.78 | ||
| Item 26 | My scalp bleeds | 0.34 | ||
| Item 16 | Water bothers my scalp | 0.54 | 0.52 | |
| Item 01 | My scalp hurts | 0.67 | ||
| Item 10 | My scalp itches | 0.69 | ||
| Item 23 | My scalp is sensitive | 0.73 | ||
| Item 07 | My scalp burns or stings | 0.74 | ||
| Item 18 | My scalp is irritated | 0.78 | ||
This table is an English translation of the Spanish version of the items comprising the Hair Specific Skindex-29.
All of the items in the questionnaire are classified as in the original questionnaire, except for slight discrepancies in 4 of them. Item 9, I worry about getting scars because of my alopecia, which is included under the emotion domain in the original scale, seems to carry greater weight in the function domain in the Spanish version. This item carries low weight in the 3domains studied (emotion, 0.3; function, 0.4; and symptom, 0.3) and would not be well differentiated in any of the 3domains; therefore, it would not greatly affect the scores on the scale.
Item 05 on the original scale, My alopecia affects my social life, is associated with the function domain, whereas in the Spanish version it could be associated with both the function domain and the emotion domain, since the values observed are very similar (weight in the function domain, 0.53 vs 0.60 in the emotion domain). The same is true of item 20, I am embarrassed by my alopecia, which is in the emotion domain in the original scale and in the function and emotion domains in the Spanish version (weight of 0.60 in the function domain vs 0.57 in the emotion domain) and with item 16, Water bothers my scalp, which is associated with the symptom domain in the original scale and also with function domain in the Spanish version. In both items, the weights of the 2 conflicting domains are similar, with the result that the items are similarly represented in both domains. Given that the difference in weight for these 4 items is minimal, the original classification of the domains is maintained for purposes of comparison with other versions of the scale.
Of the 15 patients selected for the test–retest study, all (100%) took the second test 1-2 days after the first one. No statistically significant differences were detected with respect to the overall result for Hair Specific Skindex-29, with a mean test score of 23.05 (16.42 [95% CI, 13.95-32.14]) and retest score of 22.01 (17.72 [95% CI, 17.72-12.20]). Significant differences were only observed in the emotion domain, with a decrease in the mean score of 3.67 points (5.66 [95% CI, 0.53-6.80]) in the retest (P = .02). The overall intraclass correlation coefficient was 0.98, with values greater than 0.95 in the 3domains of the questionnaire (emotion domain, 0.95; symptom domain, 0.96; and function domain, 0.97). A value greater than 0.9 is considered excellent.
DiscussionCross-cultural adaptation of an HRQOL scale to other languages requires a series of structured steps, since the translation alone is not sufficient for the instrument to be considered validated.22 Furthermore, it is necessary to evaluate the psychometric properties of the new version in a population with characteristics similar to those of the target population for the final version and to submit the instrument to a validation process in order to guarantee that it fulfills the requirements of reliability and validity necessary for this type of tool.16,23
The study of psychometric properties showed that the culturally adapted Spanish version of Hair Specific Skindex-29 made it possible to obtain statistically significant differences between healthy women and women with alopecia. The questionnaire proved fully capable of identifying the emotional impact of alopecia on patients. As expected, the highest degree of involvement was in the emotion domain, and this was already clear in women with Sinclair grade i alopecia. The degree of involvement in all the domains was directly proportional to the grade of alopecia.
Prinsen et al.24 established 2 cutoffs for each result on Skindex-29 in a sample of patients with various skin diseases. These cutoffs were set as follows: mild impact on HRQOL, 25 points; moderate impact on HRQOL, 32 points; severe impact on HRQOL, 44 points. When the data of Prinsen et al. were applied to our study, we found that the impact on the HRQOL of women with alopecia measured using Hair Specific Skindex-29 is mild to moderate, since an overall score of 26.42 points was recorded (Table 3). Prinsen et al. also determined the cutoffs for each domain on Skindex-29. As for the emotion domain, the cutoff was set at 24 points for mild emotional impact, 35 points for moderate impact, and 39 points for severe impact. In our study, the score obtained in the emotions domain of Hair Specific Skindex-29 was 36.38 points, that is, moderate to severe emotional involvement.
The study of the reliability of Hair Specific Skindex-29 shows that the tool has a high degree of reliability (Cronbach α, 0.96 [0.90 is considered to represent excellent internal consistency]) and that its discriminative power for detecting cases is extremely high, with an area under the ROC curve of 0.98.
The study of construct validity using factor analysis revealed that the items that tend to cluster according to the 3 domains, as in the original scale, and that the items that make up each domain tend to cluster consistently in each domain.
When evaluating the properties of a tool for measuring HRQOL, it is also important to evaluate its reproducibility, that is, to show that similar scores are obtained after application at 2different time points in the same population, with the same evaluators, and using the same method. The time between application of the test and the retest should not be very long in order to prevent a learning effect, that is, remembering the responses given in the first administration.25 The score obtained with Hair Specific Skindex-29 in our study did not vary significantly when the test was taken by the same patient with an interval of 1-2 days, except for the emotion domain, where the scores were statistically significantly lower in the retest than in the initial test. Nevertheless, our test–retest findings show an extremely high correlation between both tests in the 3domains, thus indicating a high degree of reliability.
ConclusionsThe cross-culturally adapted Spanish version of Hair Specific Skindex-29 proved to be a valid instrument that was sufficiently sensitive and reliable for measuring quality of life in all its domains (emotion, symptom, and function) in women with alopecia in Spain. The greatest impact was observed in the emotions domain of the questionnaire and was already present in women with Sinclair grade i alopecia. The effect on quality of life was proportional to the intensity of alopecia. Young patients were more affected in terms of quality of life, both overall and for each of the domains.
FundingThe adaptation to Spanish of Hair Specific Skindex 29was supported by a research grant from Reig Jofre.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
The Hair Specific Skindex 29 Validation Group is composed of the following dermatologists: Manuel Almagro Sánches (A Coruña), Salvador Arias Santiago (Granada), Jesús Manuel Borbujo (Madrid), Joan Escalas Taberner (Palma de Mallorca), Elena González Guerra (Madrid), Ramón Grimalt (Barcelona), Amaya Mariscal (País Vasco), M. Covadonga Martínez (Asturias), Antonio Martorell Calatayud (Valencia), José María Mir Bonafé (Palma de Mallorca), Rosa Ortega del Olmo (Granada), Juan Peris Martí (Valencia), Luis Miguel Valladares (León), and Agustín Viera Ramirez (Canarias).
The names of the members of the Hair Specific Skindex-29 validation group are listed in Appendix 1.
Please cite this article as: Guerra-Tapia A, Buendía-Eisman A, Ferrando J, 29 erdgdvHSS. Validación de una adaptación transcultural al idioma español de la escala Hair Specific Skindex-29. Actas Dermosifiliogr. 2018;109:424–431.


www.publicationethics.org.
