


To the Editor,
Primary cutaneous marginal zone lymphomas (PCMZL) are the second most common type of primary cutaneous B-cell lymphomas (PCBCL).1,2 After diagnosis, a staging workup is needed to rule out extracutaneous involvement.3 Despite being a fast, non-invasive, and inexpensive technique, cutaneous ultrasound does not have an established role in the diagnosis or follow-up of these patients. Additionally, references in the literature are scarce and based on short series of PCBCL, without any distinctions being reported across histological subtypes.
We describe two patients with PCMZL lesions, confirmed histologically, who had previously undergone ultrasound examination, with the aim of describing their ultrasonographic features. Patient #1 was a 64-year-old man with a known PCMZL and the appearance of a new lesion on the right ankle in 2021. Patient #2 was a 41-year-old woman, with no relevant past medical history, who had progressively grown a total of 9 lesions on her back and upper limbs since 2018.
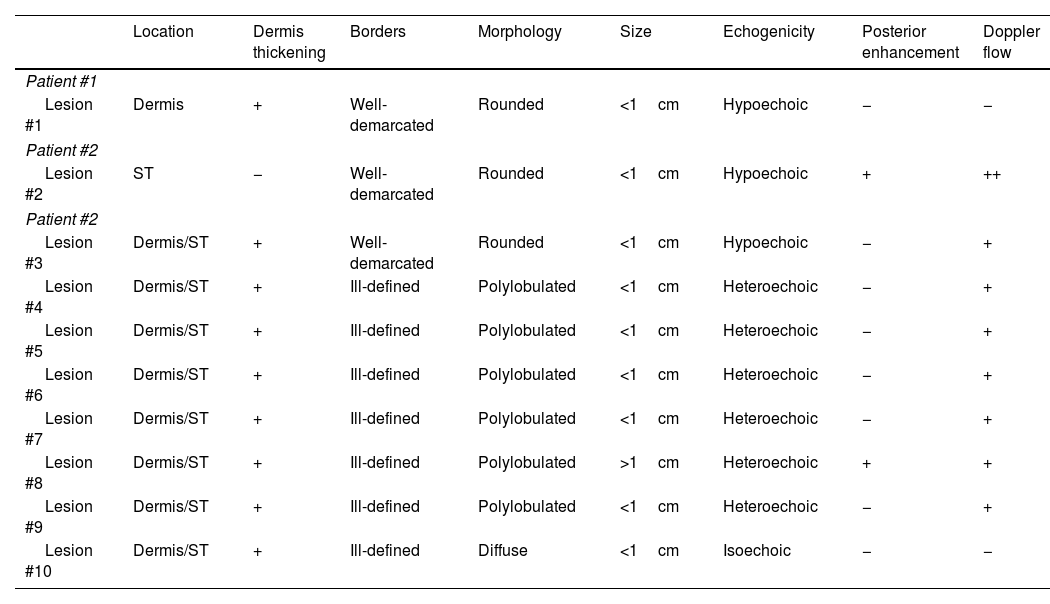
Ultrasound examinations were performed using an 18MHz probe on the Esaote Mylab™ Class C ultrasound machine. The findings are shown in Table 1. We categorized the lesions into 3 ultrasonographic patterns. Nodular pattern (3/10) included rounded lesions with well-demarcated borders and hypoechoic characteristics (Fig. 1a). Pseudonodular pattern (6/10) consisted of polylobulated lesions with poorly defined borders and heterogeneous echogenicity (Fig. 1b). The remaining lesion—showing a diffuse pattern (1/10)—was isoechoic, with poorly defined borders and a diffuse morphology (Fig. 1c).
Ultrasonic characteristics.
| Location | Dermis thickening | Borders | Morphology | Size | Echogenicity | Posterior enhancement | Doppler flow | |
|---|---|---|---|---|---|---|---|---|
| Patient #1 | ||||||||
| Lesion #1 | Dermis | + | Well-demarcated | Rounded | <1cm | Hypoechoic | − | − |
| Patient #2 | ||||||||
| Lesion #2 | ST | − | Well-demarcated | Rounded | <1cm | Hypoechoic | + | ++ |
| Patient #2 | ||||||||
| Lesion #3 | Dermis/ST | + | Well-demarcated | Rounded | <1cm | Hypoechoic | − | + |
| Lesion #4 | Dermis/ST | + | Ill-defined | Polylobulated | <1cm | Heteroechoic | − | + |
| Lesion #5 | Dermis/ST | + | Ill-defined | Polylobulated | <1cm | Heteroechoic | − | + |
| Lesion #6 | Dermis/ST | + | Ill-defined | Polylobulated | <1cm | Heteroechoic | − | + |
| Lesion #7 | Dermis/ST | + | Ill-defined | Polylobulated | <1cm | Heteroechoic | − | + |
| Lesion #8 | Dermis/ST | + | Ill-defined | Polylobulated | >1cm | Heteroechoic | + | + |
| Lesion #9 | Dermis/ST | + | Ill-defined | Polylobulated | <1cm | Heteroechoic | − | + |
| Lesion #10 | Dermis/ST | + | Ill-defined | Diffuse | <1cm | Isoechoic | − | − |
ST, subcutaneous tissue.
 Ultrasound corresponding to lesion #2, showing a hypoechoic, rounded lesion with well-demarcated borders, following a nodular pattern. Posterior enhancement and significant vascularization are also observed. (b) Ultrasound of lesion #4. In this case, a heteroechoic, polylobulated lesion with poorly defined borders, characteristic of the pseudonodular pattern, is seen. Vascularization is present but less profuse vs the previous case. (c) Ultrasound of lesion #10. This is an isoechoic, poorly defined lesion following a diffuse pattern.")
(a) Ultrasound corresponding to lesion #2, showing a hypoechoic, rounded lesion with well-demarcated borders, following a nodular pattern. Posterior enhancement and significant vascularization are also observed. (b) Ultrasound of lesion #4. In this case, a heteroechoic, polylobulated lesion with poorly defined borders, characteristic of the pseudonodular pattern, is seen. Vascularization is present but less profuse vs the previous case. (c) Ultrasound of lesion #10. This is an isoechoic, poorly defined lesion following a diffuse pattern.
In 1997, Giovagnorio4 was the first to describe the ultrasound features of various primary cutaneous lymphomas (PCL). He studied a total of 25 patients, including ten with B-cell lymphomas (BCL). He described focal and diffuse patterns, with the focal pattern being the only one observed in BCL. This pattern could further be categorized into type I (small, well-demarcated, hypoechoic nodules; 7/10) and type II (multiple well-demarcated nodules grouped into a polylobulated, hypoechoic mass; 3/10). These patterns resemble those observed in our patients: nodular pattern corresponds to Giovagnorio's type I, and pseudonodular pattern to type II, although their frequency is inverted in our series. Additionally, we observed a diffuse pattern, which was absent in Giovagnorio's BCL cases. These differences might be due to the presence of different BCL subtypes other than PCMZL in Giovagnorio's series.
In a subsequent study, Giovagnorio et al.5 described the ultrasound features of 2 BCL cases, which were rounded, well-demarcated, hypoechoic, and located in the subcutaneous tissue, with no flow on color Doppler. These lesions seem to follow a pattern similar to the nodular pattern in our series. However, they did not specify whether these were PCL or their histological subtype.
In 2019, Mandava et al.6 described the ultrasound features of PCL in 41 patients, including 33 with PCBCL. They established 4 patterns: focal infiltrative, nodular, pseudonodular, and diffuse infiltrative. Nodular and pseudonodular patterns were predominant in PCBCL—with the pseudonodular pattern being the most frequent—while the diffuse infiltrative pattern was equally observed in PCBCL and T-cell lymphomas. They also noted dermal thickening and the absence of central necrosis, calcification, or posterior acoustic shadowing in all lesions. Color Doppler flow was absent in the focal infiltrative pattern, while the other patterns were highly vascularized. Although they did not make and distinctions across histological subtypes, the ultrasonographic patterns are similar to those in our series. The main differences include inconsistent dermal thickening and vascularization in our series, although these features seem characteristic as they were present in most lesions (moreover, inconsistent flow might be due to equipment sensitivity limitations). On the other hand, posterior acoustic shadowing was observed in 2 of our cases.
Finally, in 2021, Torre-Castro et al.7 described the ultrasound features of 12 patients with PCBCL, including 3 with PCMZL. In 2 cases, ultrasound showed elongated and flattened nodules, while the remaining case showed a uninodular pattern. All lesions were found on the dermis and were well-demarcated. Vascularization was present in 2 cases, while it was scarce in the third. Lesions consisting of multiple grouped nodules would correspond to our pseudonodular pattern—although they differ in border definition—being the most common presentation of PCMZL. Additionally, the presence of variable vascularization is consistent with our observations.
The main limitation of our study is the small number of lesions analyzed from only 2 patients.
In conclusion, the ultrasound features of PCMZL are heterogeneous, with different patterns observed. The most common presentation is as polylobulated masses, followed by single hypoechoic nodules, and less commonly as diffuse thickening of the dermis and subcutaneous tissue. The scarcity of studies limits the role of ultrasound in the initial evaluation of these lesions. However, it could be useful in follow-up, particularly when new suggestive lesions appear, aiding in differential diagnosis and avoiding unnecessary biopsies.
Conflicts of interestNone declared.



