
We investigated fingers as a potential source of nickel transfer to the face in patients with allergic contact dermatitis to nickel and a history of facial dermatitis. Samples were collected from the fingers and cheeks of volunteers using the stripping method with standard adhesive tape, and nickel levels were quantified using mass spectrometry. Fingers and cheeks of individuals who had handled coins were both positive for nickel, with levels ranging from 14.67 to 58.64 ppm and 1.28 to 8.52 ppm, respectively. The levels in a control group were considerably and significantly lower. Transfer of nickel from a person's fingers to their face after handling a nickel-containing object could explain the presence of facial dermatitis in patients with nickel hypersensitivity.
Ante los casos de pacientes con historia de dermatitis facial y con dermatitis de contacto por hipersensibilidad al níquel se propuso investigar fuentes alternativas de exposición, por ejemplo monedas, que fuesen transferidas por los dedos hasta la región facial. Se utilizó cinta adhesiva común para realizar un stripping sobre los dedos y los pómulos de los voluntarios, y se llevó a cabo un análisis a través de técnicas de espectrometría atómica. Los resultados de níquel obtenidos fueron positivos tanto en los dedos, 14,67ppm a 58,64ppm, como en los pómulos, desde 1,28ppm a 8,52ppm, con niveles en controles muy inferiores y significativamente distintos a dichos valores. La transferencia de níquel desde el objeto que lo contiene hasta la cara del individuo mediante sus dedos podría justificar la clínica presentada por estos pacientes.
During the last 30 years in our skin allergy department, we have had the opportunity to examine female patients with a history of intolerance to specific cosmetic products and who were shown to have hypersensitivity to nickel in patch tests. However, searching for nickel in the products used by the patient has yielded positive results only exceptionally.1
A clear history of intolerance to metals is recorded in each case,2,3 and this finding is consistent with past relevance for nickel. Hypothetically, transfer of metal ions to the face via the fingers after contact with nickel-releasing metal objects (eg, coins,4 keys, and mobile phones5) would account for the symptoms of itching, stinging, and, in persons who are highly sensitized to nickel, the occasional finding of erythema.
The objectives of the present study were as follows: first, to confirm the transfer of nickel from coins to the fingers; and, second, to verify whether nickel can be transferred from the fingers to the face.
Material and MethodsA tape stripping method was developed to study the presence of nickel on the skin surface.6 Tape stripping involves the use of common adhesive tape not only to verify release of nickel from coins, but also to show that the nickel present on the patient's fingers7 can be transferred to the cheeks after a specific period of time. A roll of transparent adhesive tape (Niceday) measuring 19mm×33m was used to perform tape stripping, first on €1 and €2 coins and then directly on the fingers and cheeks.
The tape was cut into strips measuring approximately 5cm, which were then applied to the coins up to 10 times. The process was repeated until approximately of 1g adhesive tape was collected in a clean, sterile plastic container (Deltalab Barcelona). A blank control was created by cutting strips of tape, which were collected in another container until approximately the same weight of tape was obtained. All the samples of adhesive tape were collected in clean, sterile plastic containers until analysis.
Verification of Nickel Transfer From the Coins to the FingersThe study was performed on 10 volunteers (aged 30 to 45 years) divided into 2 groups of 5. Three were supermarket cashiers, 2 were hairdressers, and 5 were clerical workers. None of the volunteers had a clinical history of sensitization to nickel or wore prostheses or body piercings. The volunteers stopped wearing jewelry8 2 days before the test in order to avoid possible contamination of the areas studied.9
The first group had no contact with the coins. The second group rubbed the coins between their fingers for a period of 1hour. During this time, they did not wash their hands and tried not to touch any surfaces suspected of containing nickel.
Strips of Niceday tape (approximately 5cm) were cut and applied 10 times to the fingers of each of the 10 volunteers. The process was repeated until 1g of adhesive tape was obtained from each volunteer. A blank control was created by cutting strips of tape, which were collected in another container until 1g of tape was obtained. All the samples of adhesive tape were collected in clean, sterile plastic containers for analysis.
Verification of Nickel Transfer From the Fingers to the CheekThe same 10 volunteers who participated in the previous test rubbed the coins between their fingers for 30minutes and then rubbed their cheeks with the same fingers every 5minutes. Strips of transparent adhesive tape (Niceday) measuring approximately 5cm were applied the fingers of each of the volunteers 10 times. The process was repeated until 1g of adhesive tape was obtained from each volunteer. The same process was applied to collect 1g of adhesive tape from the cheeks.
In order to verify the initial absence of nickel on the fingers and cheeks, a blank control of the fingers and cheeks was created following the methodology described above.
Quantitative Analysis of NickelSamples were prepared and treated in a laboratory that was suitably prepared for determination of metals in order to avoid potential contamination. Inductively coupled plasma mass spectrometry (Agilent 7500ce) was used under standard conditions with helium. Calibration was with rhodium, which was added online as an internal standard (flow injection analysis system).
Statistical AnalysisData were analyzed using Minitab version 16.0. A descriptive analysis of the quantitative variables was performed based on measures of central tendency and dispersion. The comparative analysis was performed using the t test with a 95% confidence interval. Statistical significance was set at P<.05.
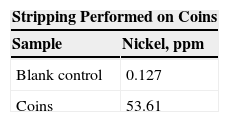
ResultsThe first test to verify release of nickel using tape stripping showed that the values obtained for the tape that had no contact with the coins were significantly lower (0.127ppm) than those of the samples used in coin stripping (53.61ppm) (Table 1).
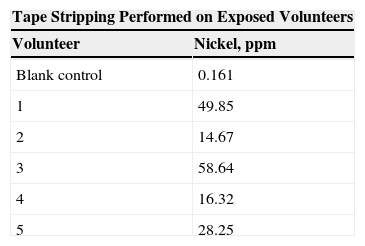
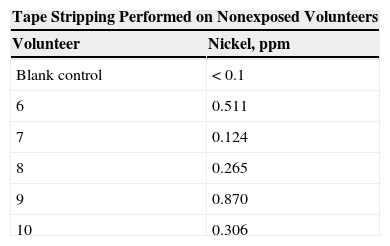
The results for verification of transfer of nickel from coins to fingers were quantifiable and differed between the groups, both when the volunteers were in contact with the coins (mean, 33.15ppm) (Table 2) and when they were not (mean, 0.41ppm) (P=.02) (Table 3).
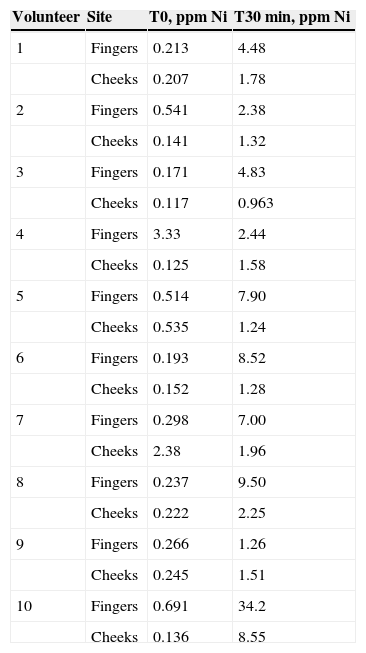
The results (Table 4) show the absence of nickel (0.6ppm on the fingers and 0.4ppm on the cheeks) before contact with coins (T0) and the presence of nickel on the fingers (mean, 8.2ppm) and cheeks (mean, 2.2ppm) after contact with coins (T30min). A statistically significant increase was observed after 30minutes, both for the fingers (P=.033) and for the cheeks (P=.035) (P<.05).
Results for Transfer of Nickel From Fingers and Cheeks After 30 Minutes’ Exposure.
| Volunteer | Site | T0, ppm Ni | T30min, ppm Ni |
|---|---|---|---|
| 1 | Fingers | 0.213 | 4.48 |
| Cheeks | 0.207 | 1.78 | |
| 2 | Fingers | 0.541 | 2.38 |
| Cheeks | 0.141 | 1.32 | |
| 3 | Fingers | 0.171 | 4.83 |
| Cheeks | 0.117 | 0.963 | |
| 4 | Fingers | 3.33 | 2.44 |
| Cheeks | 0.125 | 1.58 | |
| 5 | Fingers | 0.514 | 7.90 |
| Cheeks | 0.535 | 1.24 | |
| 6 | Fingers | 0.193 | 8.52 |
| Cheeks | 0.152 | 1.28 | |
| 7 | Fingers | 0.298 | 7.00 |
| Cheeks | 2.38 | 1.96 | |
| 8 | Fingers | 0.237 | 9.50 |
| Cheeks | 0.222 | 2.25 | |
| 9 | Fingers | 0.266 | 1.26 |
| Cheeks | 0.245 | 1.51 | |
| 10 | Fingers | 0.691 | 34.2 |
| Cheeks | 0.136 | 8.55 |
Abbreviations: Ni, nickel; T0, nickel content before exposure; T30min, nickel content after 30 minutes’ exposure.
Our findings show that contact with nickel on the fingers can lead to concentrations that are sufficiently high to cause allergic contact dermatitis via allergen transport in patients with nickel hypersensitivity. We can therefore confirm that tape stripping is a suitable method for monitoring release of nickel and that very low initial levels of nickel on the adhesive tape make it a useful material in this process.
We also confirmed transfer of nickel by contact from coins to fingers and that the nickel concentrations found are similar to those reported by other authors.10
Furthermore, we confirmed transfer of nickel from the coins to the cheeks via the fingers and showed that the differences were statistically significant. Patients 4 and 7 had increased levels of nickel on their fingers and cheeks, respectively, compared with baseline, possibly owing to contact with metal objects outside the present study that were not reported when the history was taken at inclusion. Although our study is considerably limited by its small sample size, the results are statistically significant and leave no doubt about nickel transfer and, therefore, the potentially harmful effects for susceptible individuals.
In conclusion, we show that rapid tape stripping is an easy and efficient method of demonstrating transfer of nickel via contact with coins that can be extended to other objects likely to contain nickel. This transfer could explain how dermatitis-like symptoms can be triggered on the face of very sensitive patients10 through contact with fingers exposed to nickel-releasing objects, even if these symptoms (stinging, itching) are often subjective.
Ethical DisclosuresProtection of Persons and AnimalsThe authors declare that the procedures followed adhere to the ethical guidelines of the responsible committee on human experimentation and comply with the Declaration of Helsinki of the World Medical Association.
Confidentiality of DataThe authors declare that no private patient data are disclosed in this article.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Isnardo D, Vidal J, Panyella D, Vilaplana J. Transferencia de níquel mediante los dedos. Actas Dermosifiliogr. 2015;106:e23–e26.


