
Syringomas are benign tumors of the sweat gland, primarily eccrine.1,2 Their etiopathogenesis is unknown, although a multifactorial origin is believed to exist (genetic, hormonal, frictional).3
Friedman et al. categorized syringomas into 4 groups based on their clinical characteristics: localized, generalized (which includes the eruptive form), familial, and those associated with Down syndrome.2
Eruptive syringomas are a rare variant of syringomas that appear as multiple skin-colored or slightly pigmented papules on the neck, anterior chest, axillae, or periumbilical and pubic regions, before or during puberty.1,4 Cases of eruptive syringomas have been described with involvement only in intertriginous areas, making their diagnosis even more challenging.1
A 38-year-old Caucasian woman, with a past medical history of hypothyroidism was referred to our service with a 2-year history of asymptomatic skin lesions initially appearing on her neck and chest, but later progressing over several months to involve the submammary folds, axillae, and groin. She had no family history of similar lesions.
Lesions were asymptomatic except for occasional mild pruritus and progressively increased in number, becoming an esthetic concern for the patient. She did not associate them with any trigger factors and had not received any prior treatment for this condition.
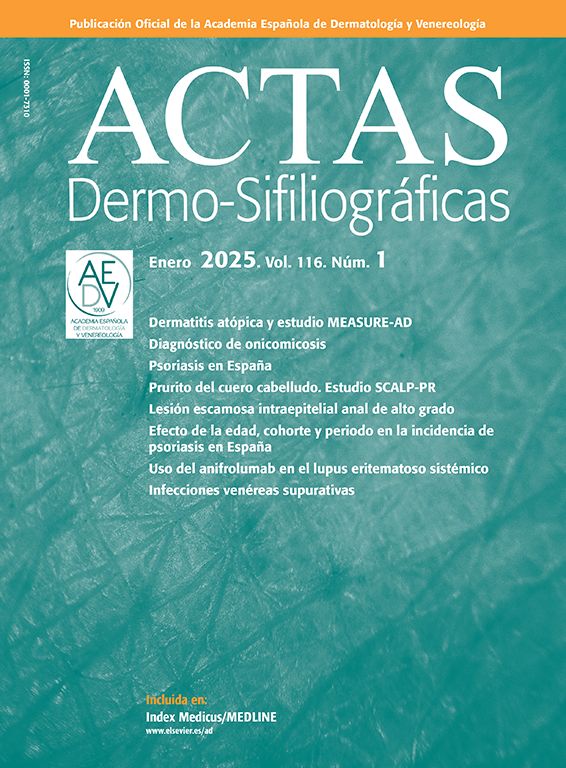
Physical examination revealed periocular papules of skin color, though notably, well-demarcated, yellow/orange papules 3–4mm in diameter, bilateral and fairly symmetrical were present in the folds (neck, axillae, groin, and submammary regions) (Fig. 1, A–D). Hair and nails were normal, with no involvement of mucous membranes.
 Multiple erythematous-yellowish, monomorphic, symmetrical papules on the neck and chest, groin, and axillae.")
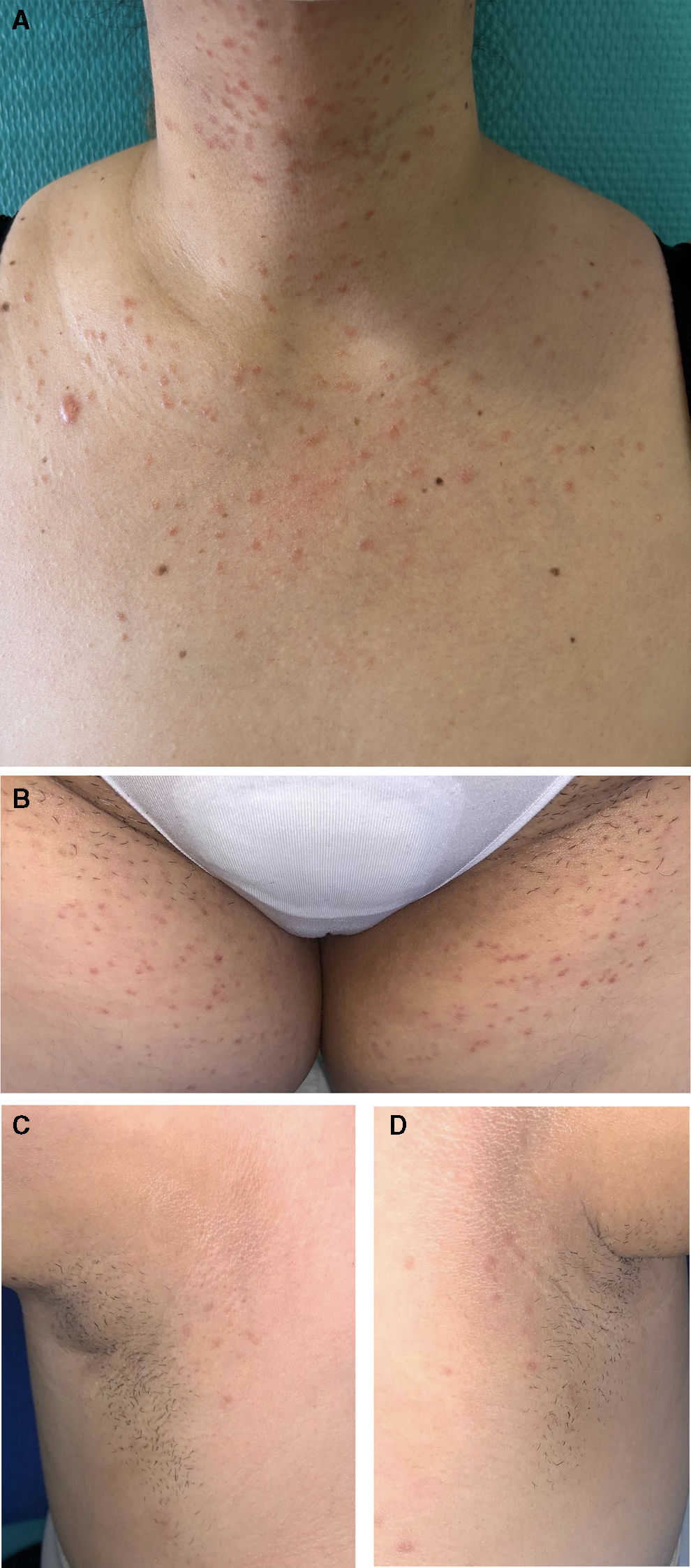
Dermoscopy showed fine brown-reddish reticulated lines on a light brown background (DermLite DL4, polarized mode, magnification ×10) (Fig. 2).

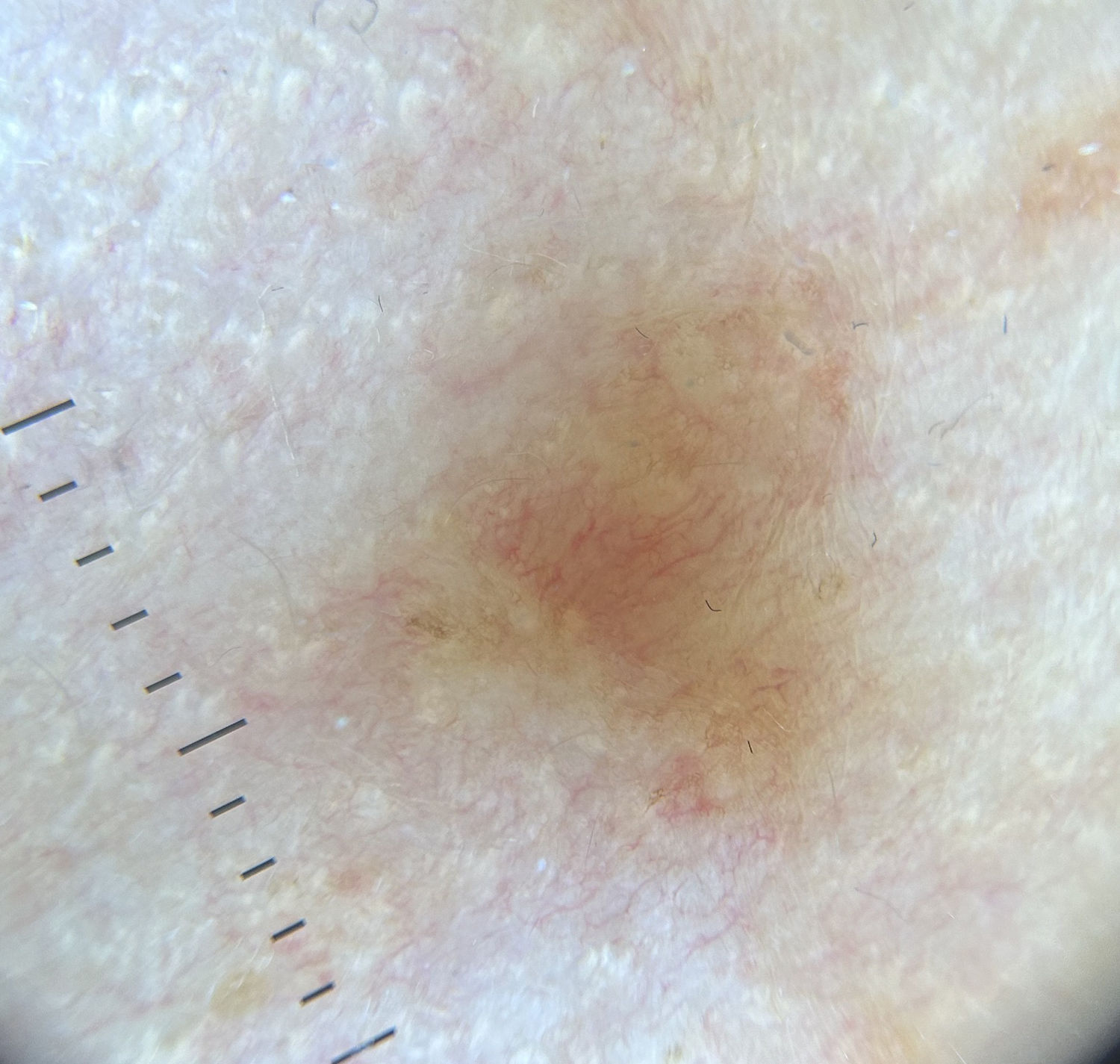
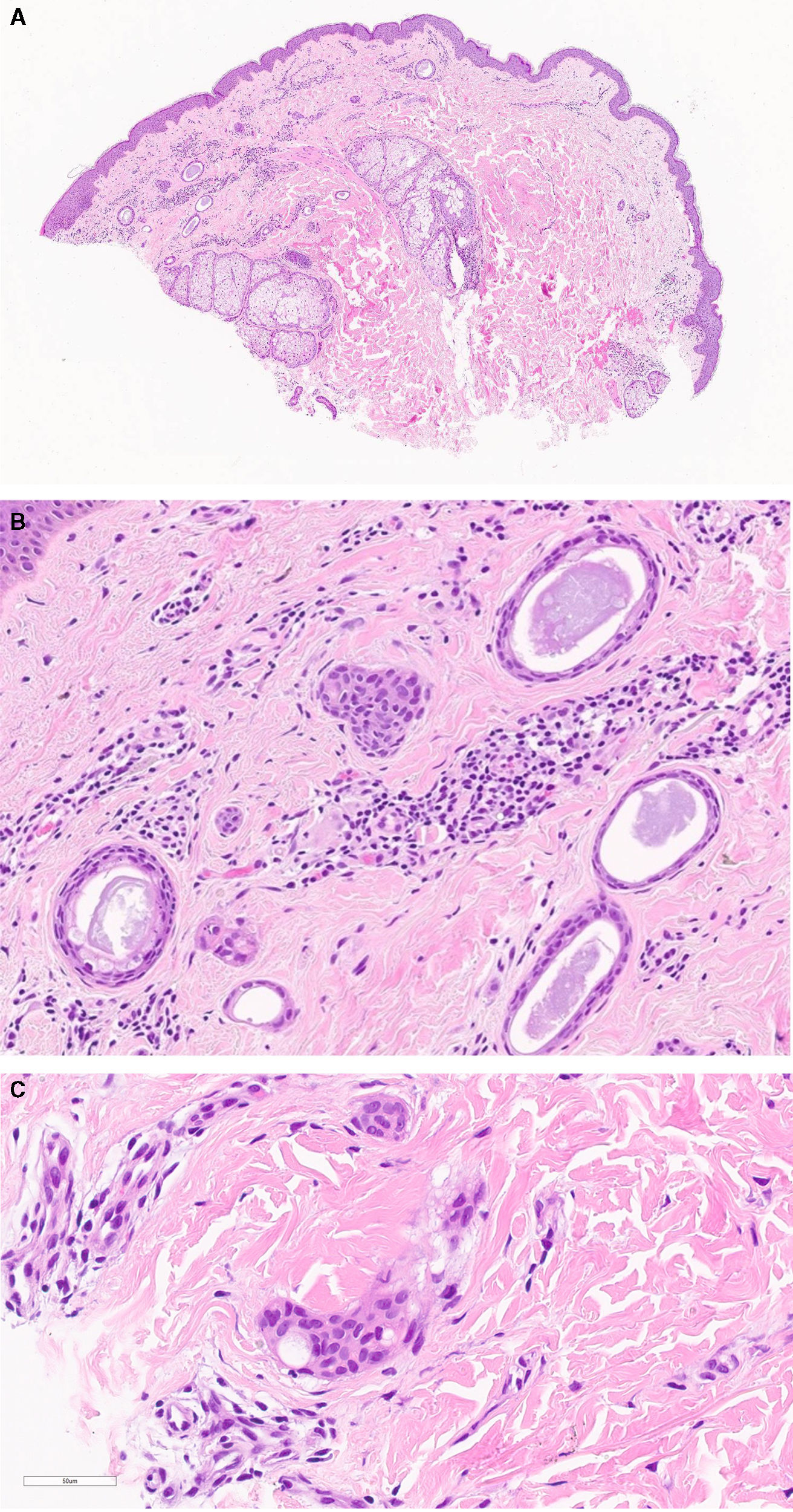
A 4-mm punch biopsy was taken, which showed a benign ductal epithelial proliferation surrounded by fibrous stroma along with a perivascular and perianexial inflammatory infiltrate on the superficial dermis, not extending any further or affecting the deep border of the biopsy. Ducts were formed by ≥1 layers of small cuboidal cells, without atypia, and some cells exhibited a tadpole-shaped configuration (Fig. 3, A–C).
 Punch biopsy showing a benign ductal epithelial proliferation, localized only in the superficial dermis. Surrounding stromal fibrosis is observed, as well as an inflammatory infiltrate with a perivascular and perianexial pattern (H&E, panoramic view). (B) At higher magnification, the lesion consists of nests and ducts formed by 1 or more layers of small cuboidal cells, without atypia (H&E ×20). (C) Occasionally, they may adopt a tadpole-like pattern (H&E ×50).")
(A) Punch biopsy showing a benign ductal epithelial proliferation, localized only in the superficial dermis. Surrounding stromal fibrosis is observed, as well as an inflammatory infiltrate with a perivascular and perianexial pattern (H&E, panoramic view). (B) At higher magnification, the lesion consists of nests and ducts formed by 1 or more layers of small cuboidal cells, without atypia (H&E ×20). (C) Occasionally, they may adopt a tadpole-like pattern (H&E ×50).
The patient's clinical picture, along with the histopathological findings, was consistent with a diagnosis of eruptive eccrine syringomas in intertriginous areas. Treatment with 10mg of oral isotretinoin daily was started, which was later up titrated to 20mg daily. However, after 6 months of treatment, the patient not only did not report improvement, but also developed more lesions, particularly on the neck and submammary folds.
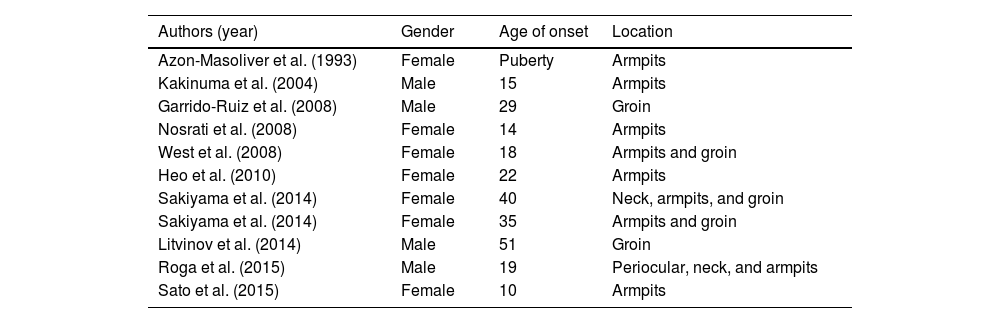
Eruptive syringomas are a diagnostic challenge as they are a rare variant affecting atypical areas.1,4 Literature reports fewer than a dozen cases of eruptive syringomas affecting only intertriginous areas (Table 1), making this presentation exceptional.3–8 In cases involving folds, the armpits are the most common location, typically with bilateral damage with involvement of both axillary and inguinal folds being extremely rare.8
Cases of eruptive syringomas.
| Authors (year) | Gender | Age of onset | Location |
|---|---|---|---|
| Azon-Masoliver et al. (1993) | Female | Puberty | Armpits |
| Kakinuma et al. (2004) | Male | 15 | Armpits |
| Garrido-Ruiz et al. (2008) | Male | 29 | Groin |
| Nosrati et al. (2008) | Female | 14 | Armpits |
| West et al. (2008) | Female | 18 | Armpits and groin |
| Heo et al. (2010) | Female | 22 | Armpits |
| Sakiyama et al. (2014) | Female | 40 | Neck, armpits, and groin |
| Sakiyama et al. (2014) | Female | 35 | Armpits and groin |
| Litvinov et al. (2014) | Male | 51 | Groin |
| Roga et al. (2015) | Male | 19 | Periocular, neck, and armpits |
| Sato et al. (2015) | Female | 10 | Armpits |
Differential diagnoses includes vulgar acne, sebaceous hyperplasia, milia, lichen planus, eruptive xanthomas, Darier's disease, pigmented urticaria, flat warts, and granuloma annulare.
Definitive diagnosis is established through histological examination, which reveals a circumscribed proliferation of ducts on the superficial dermis, formed by 2 layers of cuboidal epithelial cells, sometimes showing comma-like extensions, known as the tadpole pattern.9
Although not well defined, dermoscopu may be a useful tool, as the most widely described pattern in eruptive syringomas shows fine reticulated brown lines on a light brown background. Occasionally, white areas or points interrupt the network, corresponding to the openings of eccrine glands. Dermoscopy helps differentiate from other conditions, such as lichen planus, where white reticulated lines, also known as “Wickham's striae,” are observed.10,11
Treatment is not standardized, and many therapeutic options have been used, including topical and oral retinoids, topical atropine, cryotherapy, electrocoagulation, chemical peeling, surgical excision, and laser therapy, with generally unsatisfactory results, as seen in our patient.1,7,11,12
In conclusion, we report a new case of intertriginous eruptive syringomas, a rarely published location, although we believe these cases of syringoma may be underdiagnosed.



