

Chronic scratching is common to many skin disorders. Being a female and presenting a high level of psychopathology are risk factors for chronic scratching. Yet, it is unclear why. Certain personality characteristics that are more prevalent in women are also known to influence emotional states (i.e. emotional tension).
ObjectiveThe present study aims to explore whether these personality styles might help understand why gender and emotional distress are associated with scratching.
Material and methodsWe compared the personality patterns of 103 patients (69.9% women) diagnosed with Lichen Simplex Chronicus, against a sample of healthy individuals.
ResultsSignificant differences were found in the personality styles of men and women with LSC. Women were more pessimistic, oriented to fulfil the needs of others, traditional, insecure, submissive, and reserved, with moderate (d=.43) to strong (d=.96) size effects ranges. Some of these differences, such as in traditionalism, dutifulness, other-orientation, and pessimism, were also observed when compared with healthy men and women, with small (d=.03) to moderate (d=.47) size effects ranges.
ConclusionsThese psychological factors may help explain the mechanisms underlying gender differences in chronic scratching, at least in Lichen Simplex Chronicus. The findings might open new avenues for research and treatment.
El rascado crónico es común a varias enfermedades dermatológicas. Ser mujer y presentar niveles elevados de psicopatología son factores de riesgo para el rascado crónico. Sin embargo, aún se desconoce la causa de esta relación. Ciertas características de personalidad relacionadas con el estrés son más prevalentes en mujeres.
ObjetivoExplorar si los estilos de personalidad pueden explicar las diferencias entre hombres y mujeres en las variables psicológicas asociadas con el rascado crónico.
Material y métodosComparamos los perfiles de personalidad de 103 pacientes (69,9% mujeres) diagnosticados de liquen simple crónico y una muestra de sujetos sanos.
ResultadosSe encontraron diferencias estadísticamente significativas entre hombres y mujeres con liquen simple crónico, siendo las mujeres más pesimistas, orientadas a los demás, tradicionales, inseguras, sumisas y reservadas en cuanto a sus emociones negativas, con rangos del tamaño del efecto entre moderados (d=0,43) y altos (d=0,96). También se encontraron entre la muestra de liquen simple crónico y los controles, como por ejemplo en tradicionalismo, sumisión, orientación al otro y pesimismo, con rangos del tamaño del efecto entre bajos (d=0,03) y moderados (d=0,47).
ConclusionesEstos hallazgos podrían ayudar a explicar los mecanismos subyacentes a las diferencias de sexo en rascado crónico, al menos en el liquen simple crónico.
Some dermatologic disorders are characterized by a desire to scratch excessively, which harms the skin and delays its recovery. Researchers have tried to elucidate why excessive scratching occurs. For example, it is known that gender is a risk factor to most dermatologic diseases. Specifically, there are twice as many women with pruritic dermatological diseases compared to men.1,2 Also, women scratch more than men2 and burning process and itch sensations occur differently than in men, although no differences in specific differential pathways in the primary afferent nerves have been found.3
Together with gender differences in dermatologic diseases, increased evidence has also pointed to the importance of emotional factors in the onset and evolution of dermatologic conditions. For example, experimentally induced negative affect has been associated with increased sensitivity to itch.4 Also, perceived stress is known to be a vulnerability factor for dermatological diseases5 and itch symptoms.6 Research suggests that, as emotional tensions occur, itching and scratching increase.7 Congruent with the above, higher rates of emotional problems are found in dermatologic disorders.8 For instance, approximately one third of patients with dermatologic disorders also shows signs of psychiatric comorbidities.9 Emotional factors might also help understand gender differences in dermatologic diseases. For example, a study with 1037 patients with chronic pruritus revealed that female patients had a greater psychological burden compared to men.2 Being a female appears to be related to poorer emotional well being which, in turn, co-occurs with scratching. The question is why do women present more emotional problems and scratch behaviour?
The fact that scratch, emotional disturbance, and gender are related suggests that there might be a common underlying factor. Interestingly, personality styles are independently related to the three. First, emotional reactions and maladaptive behaviour are influenced by personality.10 In fact, personality styles have proven to be excellent predictors of health-related behaviours and emotional functioning in patients with multiple medical conditions.11–13 Second, gender differences in personality are well known. For example, research has shown that women are more other-nurturing, hesitating, and submissive than men.14 Finally, personality differences between patients with chronic itch conditions and healthy individuals have been found.15 In fact, personality styles are argued to help explain the fluctuations of skin disease by influencing emotional distress and scratching behaviour.16 Despite the above, it remains unclear whether personality styles can explain the co-occurrence of gender and emotional differences in patients with dermatologic diseases associated with chronic scratching.
Lichen Simplex Chronicus (LSC) is a prototype of a psychodermatologic disorder in which scratching is central. Patients with LSC cause or maintain inflammation (lichenification) of the skin by continuous and intense scratching, which in turn increases itch. Congruent with most psychodermatologic conditions, there are more women than men with LSC.7 Also, this disease is associated with increased psychopathology.17 In fact, its association with psychological factors is such that some psychodermatologists suggest that LSC is an emotional disorder with skin manifestations.18
The objective of the present investigation is to test whether personality styles can help to understand the higher prevalence of women and emotional problems in Lichen Simplex Chronicus, a dermatologic disease caused by scratching. We expect to find gender differences in personality styles among patients with LSC. A secondary goal is to explore whether these differences also exist between patients with LSC and healthy individuals. We hypothesize that differences in personality characteristics will occur when comparing patients with LSC and healthy individuals. Specifically, we anticipate that female patients with LSC will be more oriented to others, conforming, and focused on emotions than male participants with the disease. We expect that these characteristics will also stand out in LSC patients when compared to healthy individuals with the same gender.
Material and methodsStudy designCross-sectional with comparison group.
Study population and samplePatients diagnosed with LSC at the Dermatology Department of the Hospital Reina Sofia (Murcia, Spain) between 2010 and 2015 were included in the study. The representativity of the sample was ensured by the long recruitment period.
LSC was diagnosed based on the following inclusion criteria: one or more lichenified plaques, intense pruritus, accentuation of normal skin lines, often with a peripheral zone of closely set lichenoid papules and hyperpigmentation and/or frequent excoriation, localized in easily accessible areas, caused by repeated scratching, and in the absence of any other visible dermatological disease which justifies the itch on the LSC site. Those diagnosed with any other skin disease were excluded from the sample. In particular, patients diagnosed with atopic dermatitis or other pruritic conditions were excluded. Thus, only primary lichenification cases due to chronic scratching were included, according to the criteria of LSC.18
In order to compare some personality characteristics between the LSC group and the general population, we selected a large sample to validate the Millon Inventory of Personality Styles as the control group.19 Validation of the Millon Inventory of Personality Styles was made across 8 different geographical regions in Spain with heterogeneous demographic characteristics in order to construct a representative sample of the Spanish adult population. This strategy has been previously used in other personality studies.15,16
Assessment of personalityThe Millon Inventory of Personality Styles (MIPS) was used to assess personality styles. The MIPS evaluates three dimensions of normal personality: motivational goals, cognitive modes, and interpersonal strategies. Motivational styles evaluate the emotional goals that determine an individual's behaviour (i.e. oriented to oneself or to others). Cognitive styles assess thinking processes related to how information about the world is gathered and organized (i.e. decisions based on emotions and feelings or based on concepts and thoughts). The Interpersonal styles referred to the way a person interacts with others (i.e. submissive or dominant with others).19
The questionnaire consists of 180 true-false items divided in 24 bipolar scales (6 for motivational goals, 8 for cognitive modes, and 10 for interpersonal strategies). Although the MIPS was conceived as a personality assessment tool for general population, and not specifically in dermatological patients, it has been used to study the psychological variables that modulate the health status and to identify adaptive styles20 in relation to gender differences,14 showing good psychometric properties, and proving being a useful tool for our study.
Statistical analysisTo test whether gender differences in personality styles existed, we compared the means of men and women with LSC. In order to explore if personality styles may be risk factors for LSC, we compared the personality ratings of LSC patients with normative data on the MIPS matched by sex and age using t-tests, once the normal distribution of the personality scales were confirmed by the Kolmogorov–Smirnov test (p>.05). The effect size was evaluated by Cohen's d, a standardized mean difference index. In order to interpret the magnitudes of the d index the following cut points are usually used: small effect d=0.2, moderate effect d=0.5, and strong effect d=0.8.
EthicsThe hospital ethics committee provided ethics approval. All patients who signed the informed consent form completed the questionnaire individually and returned it to their dermatologist.
Results103 patients diagnosed with LSC (Mage=47.13 years, range 13–84, 31.1% men) and 1184 healthy-normal controls (Mage=37.60 years, range 18–65 years, 45.7% men) were included in the study.
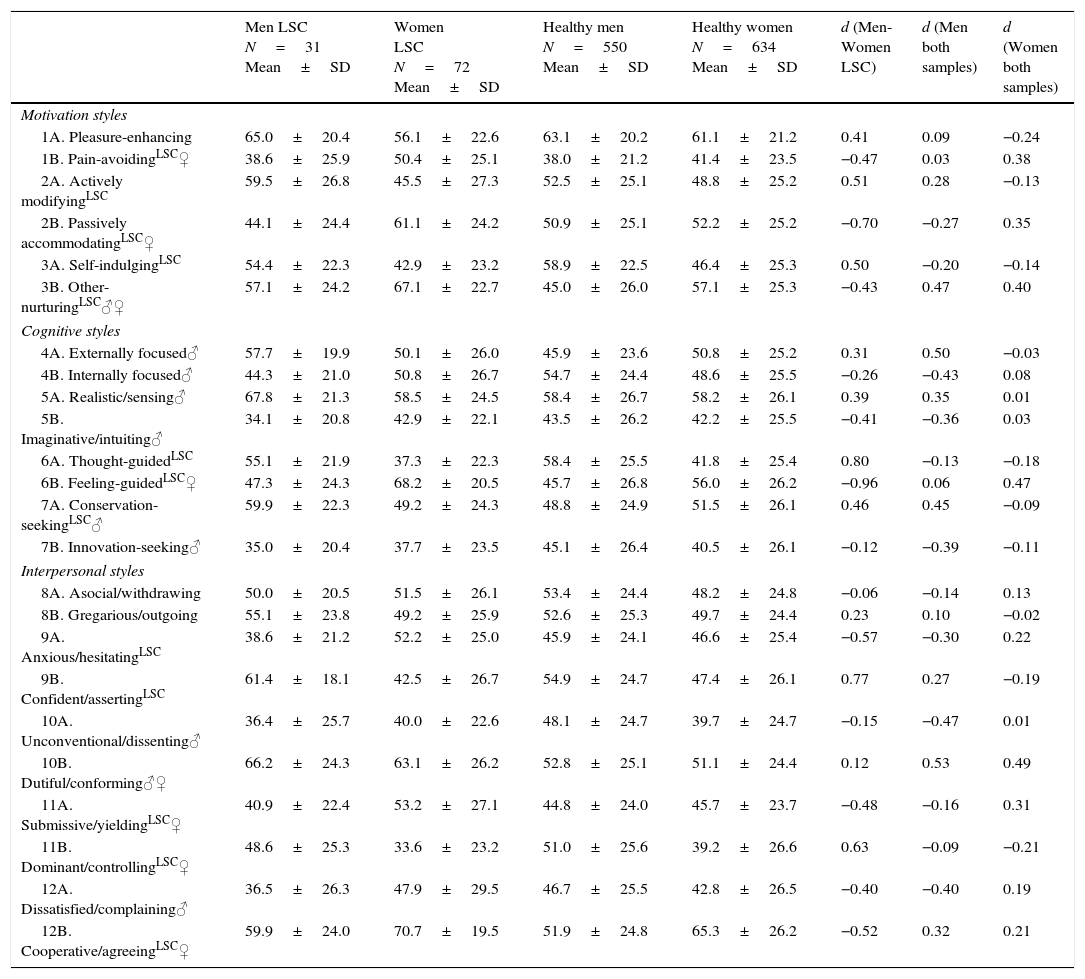
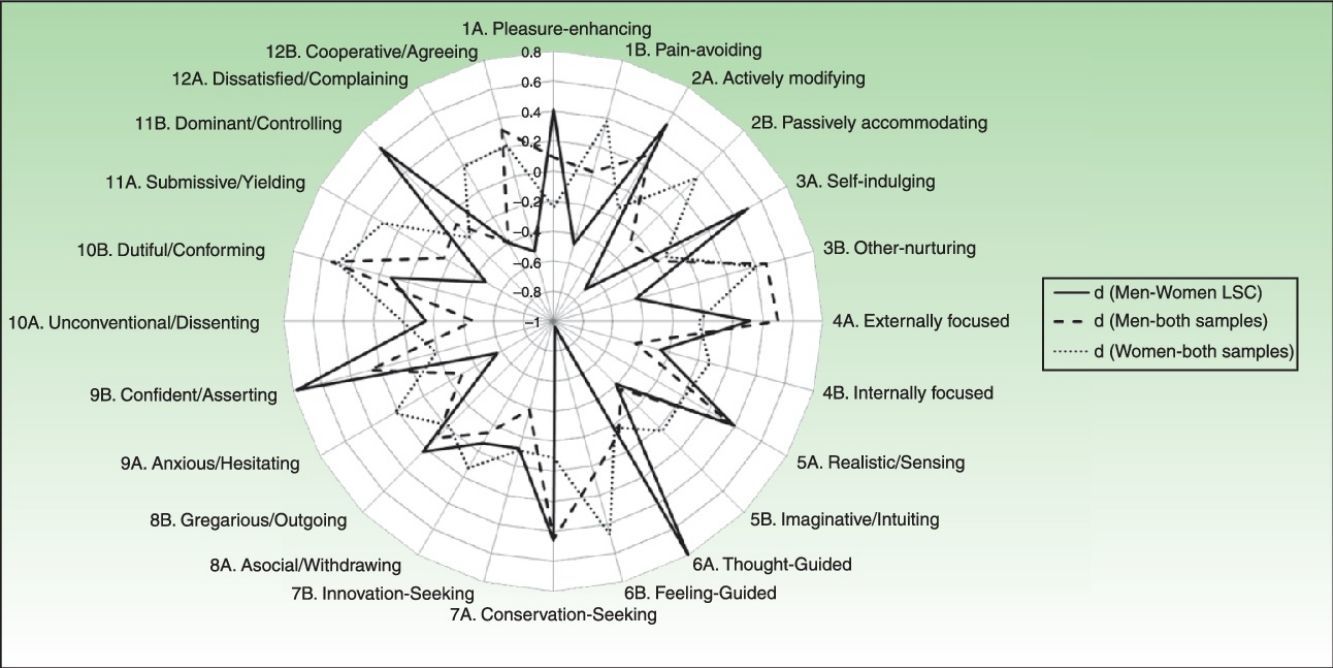
Personality differences between men and women with LSCMen and women with LSC differed in many personality styles (Table 1). Significant differences occurred in the three areas investigated: motivational goals, cognitive styles, and interpersonal strategies. Overall, women with LSC were more pessimistic, oriented to fulfil the needs of others, traditional, insecure, and submissive than men with the disease. Also, they had a higher tendency to cover their negative feelings from others. The strength of these differences ranged from moderate to strong.
Differences in means and standard deviations between men and women diagnosed with Lichen Simplex Chronicus (LSC) versus men and women without LSC. LSC Significant differences between men and women with LSC; ♂ Significant differences between men with and without LSC; ♀ Significant differences between women with and without LSC. Cohen d (standardized mean difference) was used to calculate the size effect or magnitude of the differences. Alpha level was set at 0.05.
| Men LSC N=31 Mean±SD | Women LSC N=72 Mean±SD | Healthy men N=550 Mean±SD | Healthy women N=634 Mean±SD | d (Men-Women LSC) | d (Men both samples) | d (Women both samples) | |
|---|---|---|---|---|---|---|---|
| Motivation styles | |||||||
| 1A. Pleasure-enhancing | 65.0±20.4 | 56.1±22.6 | 63.1±20.2 | 61.1±21.2 | 0.41 | 0.09 | −0.24 |
| 1B. Pain-avoidingLSC♀ | 38.6±25.9 | 50.4±25.1 | 38.0±21.2 | 41.4±23.5 | −0.47 | 0.03 | 0.38 |
| 2A. Actively modifyingLSC | 59.5±26.8 | 45.5±27.3 | 52.5±25.1 | 48.8±25.2 | 0.51 | 0.28 | −0.13 |
| 2B. Passively accommodatingLSC♀ | 44.1±24.4 | 61.1±24.2 | 50.9±25.1 | 52.2±25.2 | −0.70 | −0.27 | 0.35 |
| 3A. Self-indulgingLSC | 54.4±22.3 | 42.9±23.2 | 58.9±22.5 | 46.4±25.3 | 0.50 | −0.20 | −0.14 |
| 3B. Other-nurturingLSC♂♀ | 57.1±24.2 | 67.1±22.7 | 45.0±26.0 | 57.1±25.3 | −0.43 | 0.47 | 0.40 |
| Cognitive styles | |||||||
| 4A. Externally focused♂ | 57.7±19.9 | 50.1±26.0 | 45.9±23.6 | 50.8±25.2 | 0.31 | 0.50 | −0.03 |
| 4B. Internally focused♂ | 44.3±21.0 | 50.8±26.7 | 54.7±24.4 | 48.6±25.5 | −0.26 | −0.43 | 0.08 |
| 5A. Realistic/sensing♂ | 67.8±21.3 | 58.5±24.5 | 58.4±26.7 | 58.2±26.1 | 0.39 | 0.35 | 0.01 |
| 5B. Imaginative/intuiting♂ | 34.1±20.8 | 42.9±22.1 | 43.5±26.2 | 42.2±25.5 | −0.41 | −0.36 | 0.03 |
| 6A. Thought-guidedLSC | 55.1±21.9 | 37.3±22.3 | 58.4±25.5 | 41.8±25.4 | 0.80 | −0.13 | −0.18 |
| 6B. Feeling-guidedLSC♀ | 47.3±24.3 | 68.2±20.5 | 45.7±26.8 | 56.0±26.2 | −0.96 | 0.06 | 0.47 |
| 7A. Conservation-seekingLSC♂ | 59.9±22.3 | 49.2±24.3 | 48.8±24.9 | 51.5±26.1 | 0.46 | 0.45 | −0.09 |
| 7B. Innovation-seeking♂ | 35.0±20.4 | 37.7±23.5 | 45.1±26.4 | 40.5±26.1 | −0.12 | −0.39 | −0.11 |
| Interpersonal styles | |||||||
| 8A. Asocial/withdrawing | 50.0±20.5 | 51.5±26.1 | 53.4±24.4 | 48.2±24.8 | −0.06 | −0.14 | 0.13 |
| 8B. Gregarious/outgoing | 55.1±23.8 | 49.2±25.9 | 52.6±25.3 | 49.7±24.4 | 0.23 | 0.10 | −0.02 |
| 9A. Anxious/hesitatingLSC | 38.6±21.2 | 52.2±25.0 | 45.9±24.1 | 46.6±25.4 | −0.57 | −0.30 | 0.22 |
| 9B. Confident/assertingLSC | 61.4±18.1 | 42.5±26.7 | 54.9±24.7 | 47.4±26.1 | 0.77 | 0.27 | −0.19 |
| 10A. Unconventional/dissenting♂ | 36.4±25.7 | 40.0±22.6 | 48.1±24.7 | 39.7±24.7 | −0.15 | −0.47 | 0.01 |
| 10B. Dutiful/conforming♂♀ | 66.2±24.3 | 63.1±26.2 | 52.8±25.1 | 51.1±24.4 | 0.12 | 0.53 | 0.49 |
| 11A. Submissive/yieldingLSC♀ | 40.9±22.4 | 53.2±27.1 | 44.8±24.0 | 45.7±23.7 | −0.48 | −0.16 | 0.31 |
| 11B. Dominant/controllingLSC♀ | 48.6±25.3 | 33.6±23.2 | 51.0±25.6 | 39.2±26.6 | 0.63 | −0.09 | −0.21 |
| 12A. Dissatisfied/complaining♂ | 36.5±26.3 | 47.9±29.5 | 46.7±25.5 | 42.8±26.5 | −0.40 | −0.40 | 0.19 |
| 12B. Cooperative/agreeingLSC♀ | 59.9±24.0 | 70.7±19.5 | 51.9±24.8 | 65.3±26.2 | −0.52 | 0.32 | 0.21 |
Significant differences in personality styles were also observed between men with LSC and healthy males (Table 1). These mostly occurred in the cognitive and the interpersonal styles. In general, men with LSC were more traditional (higher score in conservative scale), more dutiful (higher score in dutiful/conforming scale), and were oriented to fulfil the needs of others than men without the disease (higher score in other-nurturing scale). They also relied more on other people than themselves for guidance. Differences were between small and moderate.
Differences between women with LSC and healthy womenLSC women also presented differences in personality when compared to healthy females, especially in motivational and interpersonal styles (Table 1). Female patients with the disease were more pessimistic, oriented to fulfil the needs of others, self-controlled, and submissive. In addition, they had a higher tendency to cover their negative feelings from others. The strength of these differences ranged from small to moderate.
DiscussionIn the light of our results, there are personality differences between male and female patients with LSC, and also when they are compared with healthy individuals. Some, personality styles that are more frequent in females might be relevant risk factors for the chronic course of LSC. For example, women with LSC showed an increased tendency to be guided by feelings and emotions rather than by objective information when coping with stress. Surprisingly, they reported frequently hiding their negative emotions in order to cooperate and be in agreement with others. Congruent with these findings, previous research has revealed that women suppress the expression of emotions that they consider to be inconsistent with their gender role,21 mainly aggression.22 Most importantly, the use of this coping seems to reduce the ability to solve interpersonal conflicts,23 possibly by increasing physiological arousal, and subjective states of emotional distress.24 The above seems to hold true for patients with LSC, who present increased emotionality, difficulties in regulating their emotions and high levels of psychopathology.
Support for a stronger relationship between tension and scratching for women comes from those studies showing that emotional distress and psychopathology are associated with itching and scratching, and the link is stronger for women.25,26 A relationship between stress and negative emotions is well established. For example, stressful situations have been associated with numerous negative emotions (i.e. anger, anxiety and depression). In LSC, scratching might be one form of reducing stress. Even though this is arguably a maladaptive form of coping with stress, the use of such coping efforts in front of stress is not new. Self-mutilation, for example, is a well-known form of passive coping.27 These findings suggest that intense scratching, as shown in LSC, could act as a mild form of self-aggression. This might be one way of coping with stress in the absence of a better strategy to deal with emotional tension and increased arousal. Because personality styles tend to remain stable, when these styles are maladaptive scratching may become chronic.
Our results suggest that the aforementioned pathway might be especially relevant for females. Personality differences in our study might explain, at least to some extent, the higher prevalence of women with chronic scratching. Interestingly, some of these differences also occurred in men with LSC, although only partially and in lower magnitude. For example, men with LSC were more other-oriented, less dissenting, more dutiful, and less complaining compared to healthy males. Therefore, these personality styles might not only be risk factors for the LSC in women, but for men. Another important finding in our study was that some personality differences between LSC patients and healthy individuals were gender-specific. While men differed in cognitive styles, women mostly differed in motivational styles. The components of interpersonal styles in which LSC patients and healthy individuals differed depend on gender too. This makes us think that different pathways might be intervening in chronic scratching, at least in LSC.
In the previous paragraph we noted that certain personality styles might be considered to be risk factors for LSC only in males. For example, men with the disease prefer objective information and other people's opinions than their own intuitions and thoughts for guidance (realistic vs. imaginative and externally vs. internally focused). In addition, LSC males are more traditional and systematic in the way they gather information, in opposition to creative and novelty seeking (conservation vs. innovation). In line with this, they report following traditional social standards (unconventional) and being very stable in the way they think, feel and behave (dissatisfied). In this sense, a research has revealed that men tend to be more rigid in the way they think and behave, and this rigidity is associated with psychopathology.28 This might explain why this personality profile was more prominent in males with LSC in our sample.
This study certainly has some limitations. First of all, we used a cross-sectional design, which prevents us from drawing causal conclusions. That is, even if we found personality differences between LSC patients and healthy individuals, we cannot be sure that these personality styles are responsible for the onset of pathology. However, prospective research has shown this might be the case for many diseases.29 Moreover, even if emotional reactions involved in LSC are partly attributable to certain personality styles, the relation between these and scratching remains unexplored. The fact that certain personality styles were more prevalent in people who scratch does not necessarily mean that one caused the other. For example, negative affective states (such as anxiety, depression or anger), a possible confounding variable, was not measured. In addition, the severity of the lesion, economic status, family disturbances, etc., could also trigger or maintain scratching behaviour and should be taken into account in future studies. It is also important to note that, although LSC is a good model of chronic scratching, our findings are not necessarily generalizable to other dermatological conditions. Another limitation of the current investigation is that the control group used for personality comparison was a sample collected in a previous investigation in which the existence of dermatologic or mental problems was not assessed. While acknowledging this shortcoming, the sample assessed in the validation of the Millon Inventory of Personality Styles used a large population representative of the general population of Spain19; therefore, the present results may serve as indicators of personality differences between patients with LSC and people from the general population in Spain.
In summary, the present study suggests that personality styles should not be overlooked in the context of LSC, both in males and females. Our results suggest that certain adaptive styles increase the likelihood of behavioural responses (i.e. scratching) to stress through experiencing stressful situations and using maladaptive emotional regulation strategies (i.e. emotional suppression of unexpressed tension). As the specific mechanisms through which psychological variables influence the desire to scratch remain speculative, more studies addressing gender differences in personality should be carried out in dermatologic patients with chronic scratch behaviour. Moreover, we recommend assessing personality, especially in women, in order to detect patients with a higher risk of developing chronic scratching conditions. We suggest that the evaluation of personality should help to guide the treatment of patients with dermatologic conditions in which scratching is important.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestThe authors declare that they have no conflict of interest.


