








Melanocytic nevi are frequently found on acral volar skin. Differentiation between nevi and melanoma is essential and sometimes difficult, although dermoscopy has enabled a more specific diagnosis of pigmented lesions. Dermoscopic patterns of lesions on acral volar skin have mostly been described in European and Asian populations. The Latin American population is heterogeneous, and particularly so in the case of Uruguayans, who largely descend from 3 distinct populations.
ObjectiveTo describe dermoscopic patterns of acral melanocytic nevi and evaluate their applicability in a Latin American population in Uruguay.
Patients and MethodsThis was an observational, descriptive, cross-sectional study conducted by 2 dermatologists from 4 dermatology clinics in Uruguay. Uruguayan patients older than 18 years with acral melanocytic nevi were included. Digital dermoscopic images were captured and jointly analyzed by 2 investigators.
ResultsA total of 158 acral volar nevi in 80 patients were analyzed. The most-prevalent pattern was the parallel furrow pattern (51.3% of nevi), followed by the latticelike pattern (13.3%), the homogeneous pattern (12.7%), the globular pattern (9.5%), the fibrillar pattern (7%), the globulostreaklike pattern (3.8%), and the nontypical pattern (2.5%). The reticular and transition patterns were not observed in our population.
ConclusionsThe parallel furrow pattern, followed by the latticelike and homogeneous patterns, was the most-prevalent pattern in acral melanocytic nevi in the Uruguayan population. The fibrillar pattern was found exclusively on the soles. No new dermoscopic patterns were observed. The patterns described in Asian and European literature apply to our population.
Los nevos melanocíticos se encuentran con frecuencia en la piel volar acral. La diferenciación entre nevos y melanoma es imprescindible y a veces difícil, aunque la dermatoscopia ha permitido un diagnóstico más preciso de lesiones pigmentadas. Los patrones dermatoscópicos de lesiones en la piel volar acral han sido descritos en su mayoría en poblaciones europeas y asiáticas. La población latinoamericana es heterogénea, y en particular en el caso de los uruguayos, que provienen en gran parte de 3 distintas poblaciones.
ObjetivoDescribir los patrones dermatoscópicos de nevos melanocíticos acrales y evaluar su aplicabilidad en una población latinoamericana en Uruguay.
Pacientes y métodosSe trata de un estudio observacional, descriptivo y transversal realizado por 2 dermatólogos de 4 clínicas dermatológicas en Uruguay. Se incluyeron pacientes mayores de 18 años con nevos melanocíticos acrales. Las imágenes dermatoscópicas fueron captadas y analizadas de forma conjunta por 2 investigadores.
ResultadosUn total de 158 nevos volares acrales en 80 pacientes fueron analizados. El patrón más frecuente fue el patrón paralelo del surco (51,3% de los nevos), seguido por el patrón en celosía (13,3%), el patrón homogéneo (12,7%), el patrón globular (9,5%), el patrón fibrilar (7%), el patrón retículo-globular (3,8%), y el patrón atípico (2,5%). No se observaron los patrones reticular y de transición en nuestra población.
ConclusionesEl patrón paralelo del surco, seguido por los patrones en celosía y homogéneo, fueron los más frecuentes en nevos melanocíticos acrales en la población uruguaya. El patrón fibrilar se encuentra exclusivamente en las plantas de los pies. No se observaron nuevos patrones dermatoscópicos. Los patrones descritos en la literatura asiática y europea son aplicables a nuestra población.
The incidence of acral melanoma, at 0.3 cases per 100000 inhabitants per year,1 has been reported as being virtually identical in all ethnic groups, including whites.1,2 Acral volar skin is the most common site of malignant melanoma in non-whites,1–7 and in the white population, acral melanoma accounts for about 4.5–7% of all melanomas.4,8 Prognosis is generally poor, primarily due to the delay in detection.2,9,10 Early diagnosis and treatment are thus essential to improve survival.1,2,7
Considering that melanocytic nevi are frequently found on acral volar skin,1 it is essential to differentiate between nevi and melanoma. An accurate diagnosis, however, is difficult by simple visual inspection. Dermoscopy has emerged as a noninvasive technique that aids the clinical diagnosis of pigmented skin lesions, offering improved sensitivity and specificity.4,5,7,8,11
Most dermoscopic patterns described in acral volar skin to date have been studied in European and Asian populations, and consist of the parallel furrow pattern with its variants, latticelike, fibrillar, nontypical, globular, homogeneous, reticular, transition, and globulostreaklike patterns.1,4–6,11–14 Four patterns are suggestive of melanoma in acral volar skin: the parallel ridge pattern, irregular diffuse pigmentation, the serrated pattern, and the multicomponent pattern.4,8,15
The Uruguayan population is heterogeneous; most of the population is of European descent (mainly Spanish and Italian), but there are also people of indigenous (1–20%) and African (7–15%) descent.16,17
The aim of this study was to describe the dermoscopic patterns of acral melanocytic nevi and evaluate their applicability to a Latin American population of Uruguay.
Patients and MethodsThis observational, descriptive, and cross-sectional study was conducted by 2 dermatologists in 4 dermatology clinics in Uruguay, including 3 teaching hospitals (Hospital de Clínicas, Hospital Las Piedras, and Hospital Español) and 1 private center (Medicina Personalizada), between January 2010 and January 2011.
Inclusion criteria were an age of over 18 years, Uruguayan nationality, consultation in a dermatology office for any cause, and the presence of at least 1 acral nevus diagnosed both clinically and dermoscopically. Patients were included consecutively. Lesions in dorsal and subungual areas were excluded. Exclusion criteria were the presence of melanocytic lesions on acral volar skin with dermoscopic features indicative of melanoma.
For each patient we collected data of the predominant body pattern of the nevi, the number of volar lesions, dermoscopic patterns, and the location and diameter of each volar lesion. Locations on the palms were schematically divided into 4 categories: thenar eminence, hypothenar eminence, volar aspect of digits, and rest of the palm. Locations on the soles were divided into arch, heel, volar aspect of the digits, external aspect of the sole, and the metatarsal sole area.
Digital dermoscopic images were captured with a Canon PowerShot A630 digital camera equipped with a Dermlite Foto dermoscope and a digital epiluminescence microscope system (FotoFinder medicam 500, Fotofinder Systems 2007).
All the images were jointly evaluated by 2 dermatologists. The patterns were classified according to the 9 patterns described in the literature: parallel furrow, latticelike, fibrillar, nontypical, homogeneous, globular, reticular, transition, and globulostreaklike.1,4–6,11–14 Following the criteria described by Saida et al.5 for nevi that show a combination of 2 or 3 patterns, we considered the predominant pattern in each case. Skin types were classified according to Fitzpatrick's phototypes.
Descriptive statistical analysis was performed with SPSS version 15.0.
ResultsEighty Uruguayan patients (61 women and 19 men) with melanocytic nevi located on acral volar skin were included. Their mean (SD) age was 35.6 (13.3) years old. Thirty-one patients (38.8%) had skin type II, 31 (38.8%) skin type III, 11 (13.8%) skin type IV, and 1 (1.3%) skin type VI. The most common predominant body pattern of melanocytic nevi was reticular (39 patients, 48.8%), followed by reticular-globular (10 patients, 12.5%) and reticular-homogeneous (8 patients, 10%).
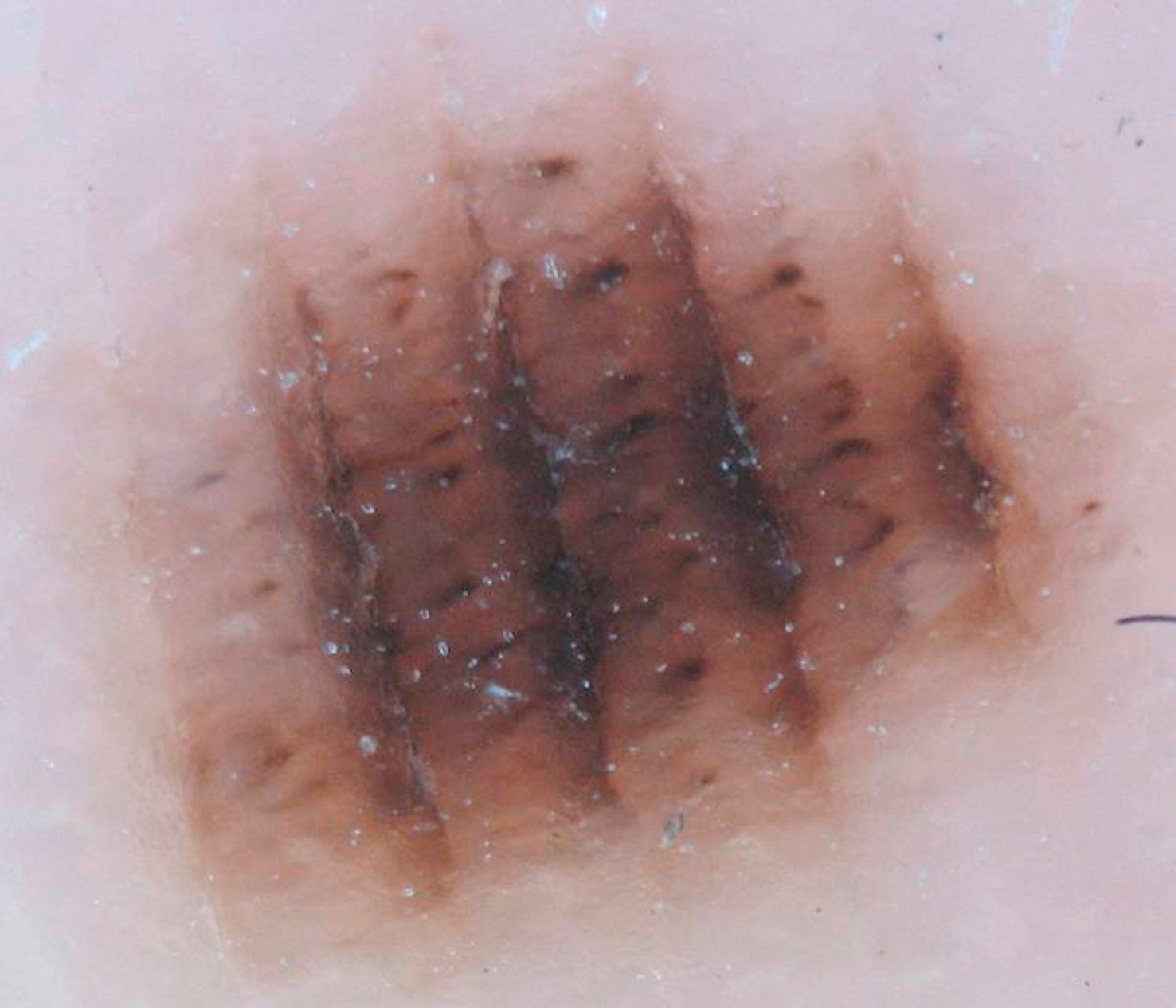
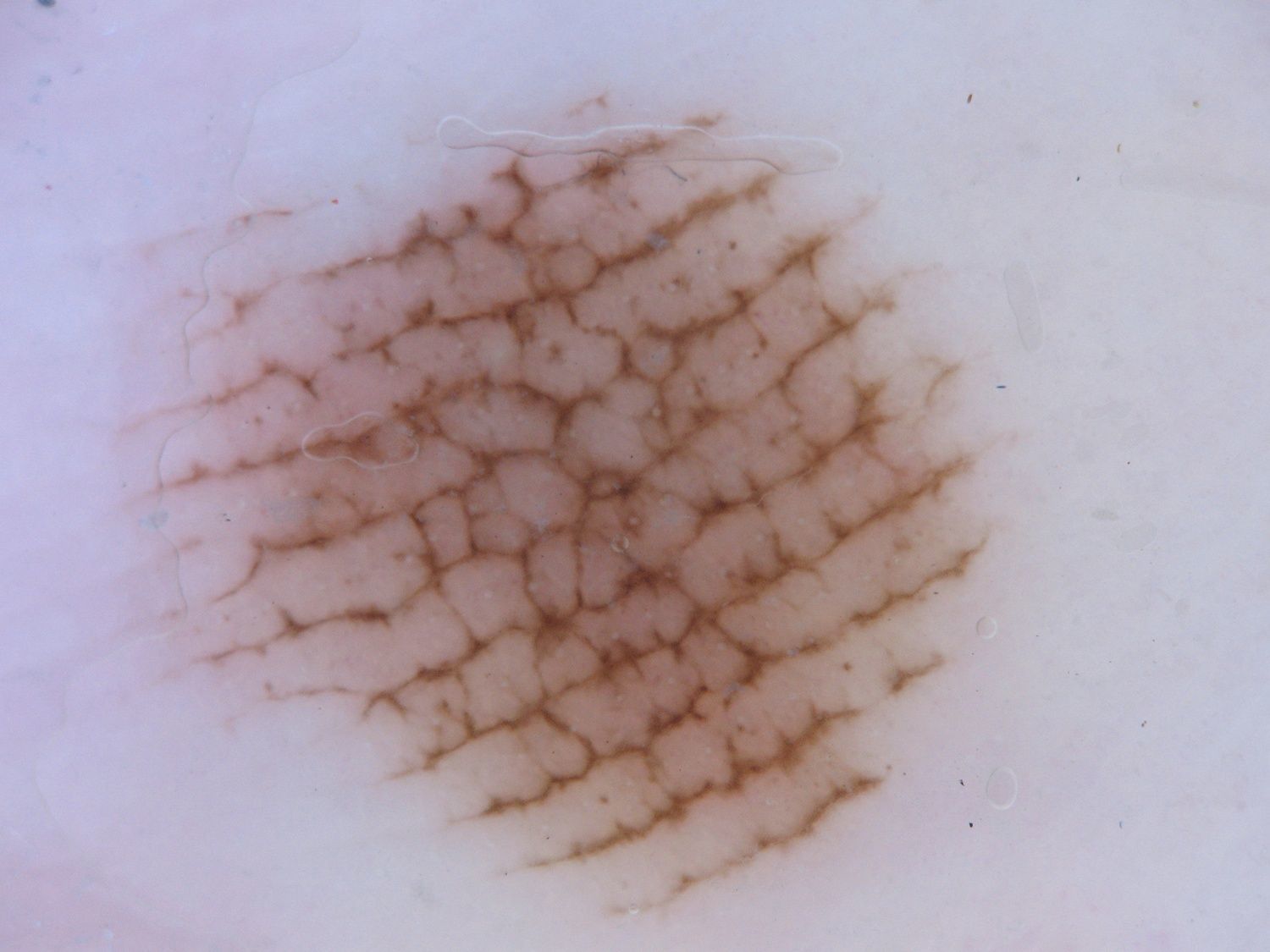
In total, 158 acral volar nevi from 80 patients were analyzed. The mean number of nevi per patient was 2 (1.3) and the mean diameter of lesions was 2.5 (1.7)mm. According to the 3-step algorithm for the management of acquired acral melanocytic lesions,2 3 lesions measuring 8 and 9mm in diameter were biopsied in 3 patients. They corresponded to acquired acral melanocytic nevi on the sole. The rest of the lesions will be monitored as necessary. The most prevalent dermoscopic pattern was the parallel furrow pattern, observed in 81 nevi (51.3%) (Figs. 1–4). This was followed by the latticelike pattern (n=21, 13.3%) (Fig. 5), the homogeneous pattern (n=20, 12.7%), the globular pattern (n=15, 9.5%), the fibrillar pattern (n=11, 7%) (Fig. 6), the globulostreaklike pattern (n=6, 3.8%) and the nontypical pattern (n=4, 2.5%). There were no cases of the reticular or transition pattern, and all the patterns observed had been previously described.




The nevi were located on the palms in 81 patients (51.3%) and on the soles in 77 patients (58.7%). On the palms, 33 nevi (20.9%) were located on the palmar aspect of the digits, 18 (11.4%) on the thenar eminence, 16 (10.1%) in the center of the palm, and 14 (8.9%) on the hypothenar eminence. The parallel furrow pattern was the most common pattern in all locations. None of the nevi on the palms exhibited a fibrillar pattern.
On the soles, 28 nevi (17.7%) were located on the arch, 20 (12.7%) on the external aspect of the sole, 16 (10.1%) on the volar aspect of the digits, 8 (5.1%) on the heels, and 5 (3.2%) in the metatarsal sole area. The parallel furrow pattern was also the most common pattern in all locations (n=36, 46.7%) except the heel, where it was the fibrillar pattern. Table 1 summarizes the distribution of dermoscopic patterns according to the anatomical site of the lesion.
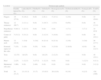
Dermoscopic patterns in different acral locations.
| Location | Dermoscopic pattern | |||||||
| Parallel furrowNo. (%) | LatticelikeNo. (%) | FibrillarNo. (%) | GlobularNo. (%) | HomogeneousNo. (%) | GlobulostreaklikeNo. (%) | NontypicalNo. (%) | TotalNo. (%) | |
| Fingers | 19 (57.6) | 6 (18.2) | 0 (0) | 2 (6.1) | 5 (15.1) | 1 (3.0) | 0 (0) | 33 (20.8) |
| Thenar eminence | 12 (66.7) | 2 (11.1) | 0 (0) | 3 (16.7) | 1 (5.5) | 0 (0%) | 0 (0) | 18 (11.4) |
| Hypothenar eminence | 9 (64.3) | 3 (21.5) | 0 (0) | 0 (0) | 0 (0) | 1 (7.1) | 1 (7.1) | 14 (8.9) |
| Center of palm | 5 (31.2) | 5 (31.2) | 0 (0) | 2 (12.5) | 3 (18.8) | 1 (6.3) | 0 (0) | 16 (10.1) |
| Plantar arch | 12 (42.8) | 1 (3.6) | 1 (3.6) | 6 (21.4) | 6 (21.4) | 1 (3.6) | 1 (3.6) | 28 (17.7) |
| External aspect of the soles | 7 (35) | 2 (10) | 5 (25) | 0 (0) | 3 (15.0) | 2 (10.0) | 1(5.0) | 20 (12.7) |
| Toes | 12 (75) | 1(6.25) | 0 (0) | 1(6.25) | 2 (12.5) | 0 (0) | 0 (0) | 16 (10.1) |
| Heel | 2 (25) | 1 (12.5) | 3 (37.5) | 1 (12.5) | 0 (0) | 0 (0) | 1 (12.5) | 8 (5.1) |
| Metatarsal sole area | 3 (60) | 0 (0) | 2 (40) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 5 (3.2) |
| Total | 81 (51.3) | 21 (13.3) | 11 (7) | 15 (9.5) | 20 (12.6) | 6 (3.8) | 4 (2.5) | 158 (100) |
The dermoscopic patterns found in this study of Latin American patients with acral melanocytic nevi are similar to those described in Asian and European populations, probably because pigment distribution in the palms and soles is similar across races.
The anatomical structure of acral volar skin results in unique dermoscopic features in this location.4,12 Dermoscopic studies of nevi and melanomas located on the palms and soles were first performed by Japanese authors, who proved the utility of dermoscopy in this setting.5,7,8,11 Saida et al.13 had examined acral nevi in the Asian population. They were pioneers in describing specific dermoscopic patterns, including the parallel furrow pattern with its variants, where pigmentation is seen in the parallel sulci of the skin markings; the latticelike pattern, characterized by pigmented lines that follow and cross the skin markings; the fibrillar pattern, consisting of pigmented lines that cross the skin markings diagonally; and the nontypical pattern.1,4–6,11,13 This last pattern is used to describe acral melanocytic lesions that show neither malignant features nor the benign patterns described above on dermoscopy.4 Three additional dermoscopic patterns, namely the globular pattern (brown globules regularly distributed within the lesion), the homogeneous pattern (diffuse light brown or blue pigmentation), and the reticular pattern (black or brown network similar to that seen in nonglabrous skin), were subsequently described in patients with atypical mole syndrome.4,5,8,11 This dermoscopic classification was also applied to a white population in central Italy.12 Later studies described a transition pattern, consisting of a combination of specific dermoscopic features characteristic of volar and nonglabrous skin.5,12 In 2007, a globulostreaklike pattern which exhibited dark brown globules and brown linear or curvilinear streaklike structures was described.4,14
We found a mean of 2 acral nevi per patient in our population, which seems to be high as compared with other studies performed in Spain (Barcelona),8 central Italy,11 and Turkey.14 This could be explained by differences in study design, particularly with respect to inclusion criteria. In our series, we included only patients with at least 1 acral nevus, whereas in the other studies patients were included regardless of whether or not they had acral nevi.
Our findings are consistent with reports in the literature in that the most prevalent pattern of acral melanocytic nevi was the parallel furrow pattern, accounting for 51.3% of lesions. The prevalence of this pattern in other reports ranges from 42% to 59% depending on the population analyzed.5,8,11,14 The second-most common pattern in our series was the latticelike pattern (13.3%), which is consistent with figures of between 13% and 15% reported for populations in Japan,5 Spain,8 and Italy.11 Ozdemir et al.5 in contrast, have reported a prevalence of just 7% in the Turkish population. Although the frequency of the latticelike pattern in the Japanese population was similar to that reported in Spaniards, Italians, and Uruguayans, this pattern was the third-most common one in the Japanese series.5 The third-most common pattern in our population—the homogeneous pattern—was found in 12.7% of patients. This appears to be much higher that frequencies reported in other populations (2–9%), particularly in the Japanese, and is possibly related to ethnic differences.5 The globular pattern, observed in 9.5% of nevi, occupied fourth place in our series, again differing from other studies, which have reported variable rates of 2% to 5%, with this pattern occupying fourth, fifth and sixth places.5,8,11,14 The fibrillar pattern was observed in 7% of lesions, which is similar to the figure reported by Malvehy and Puig8 in Spain, although prevalence rates in the literature vary between 6% and 21%. None of the nevi we examined exhibited the reticular or transition pattern. The prevalence of the globulostreaklike pattern, and the nontypical pattern in particular, was low as compared with other studies, but this might due to interobserver variability.
The absence of new dermoscopic patterns confirms the applicability of previously described patterns in our population. Table 2 summarizes the frequencies reported in the studies cited in this article. Nonetheless, caution should be exercised when comparing results between dissimilar populations, and it should also be noted that new acral patterns have been discovered through the years.
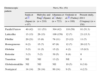
Prevalence of dermoscopic patterns in acral melanocytic nevi in different studies.
| Dermoscopic pattern | Nevi, No. (%) | ||||
| Saida et al.15 (Japan) (n=97) | Malvehy and Puig5 (Spain) (n=210) | Altamura et al.7 (Italy) (n=723) | Ozdemir et al.10 (Turkey) (n=188) | Present study, 2011 (Uruguay) (n=158) | |
| Parallel Furrow | 40 (42) | 111 (53) | 304 (42) | 110 (59) | 81 (51.3) |
| Latticelike | 13 (13) | 26 (13) | 108 (159) | 12 (7) | 21 (13.3) |
| Fibrillar | 20 (21) | 13 (6) | 78 (11) | 23 (12) | 11 (7) |
| Homogeneous | 8 (2) | 15 (7) | 67 (9) | 12 (7) | 20 (12.7) |
| Globular | 5 (5) | 11 (5) | 15 (2) | 4 (2) | 15 (9.5) |
| Reticular | 3 (3) | 5 (2) | 39 (5) | 8 (4) | 0 |
| Transition | NE | NE | 13 (2) | NE | 0 |
| Globulostreaklike | NE | NE | NE | 10 (5) | 6 (3.8) |
| Nontypical | 14 (14) | 29 (14) | 99 (14) | 9 (5) | 4 (2.5) |
Abbreviation: NE, not evaluated.
Although the fibrillar pattern was the second-most common pattern found on the soles, it was absent from the palms, as described by Altamura et al.11 This pattern is found most frequently in weight-bearing areas, and in fact, it seems that high pressure points and shearing forces contribute to the dermoscopic features of this pattern.18,19 This may explain why we did not find the fibrillar pattern on the palms and also possibly why it was so common on the heel and the external aspect of the soles and in the metatarsal sole area.
In our opinion, the differences found in the studies analyzed could have multiple explanations. The main limitation with our study is that we studied a small number of lesions in a sample of Latin Americans exclusively from Uruguay. Ethnic differences and interobserver variability may account for variations in pattern prevalence between different studies. Furthermore, some nevi show a combination of 2 or 3 patterns in the same lesion, and classification criteria could thus vary according to the examiner.
Dermoscopy is a powerful tool for discriminating between acral nevi and early acral melanoma. The recognition of dermoscopic patterns of melanocytic lesions is essential, as both melanoma and acral nevi present clinically as small, uniformly pigmented macules.20
To the best of our knowledge, this is the first study of dermoscopic patterns of acral nevi in Latin America. The patterns observed are similar to those described in Asian and European populations. Accordingly, our study could contribute to the recognition of benign acral patterns and show their applicability in Latin American patients.
Ethical DisclosuresProtection of Human and Animal SubjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of DataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to Privacy and Informed ConsentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Barquet V, Dufrechou L, Nicoletti S, Acosta M, Magliano J, Martínez M, et al. Patrones dermatoscópicos de 158 nevos melanocíticos acrales en una población latinoamericana. Actas Dermosifiliogr. 2012. http://dx.doi.org/10.1016/j.ad.2013.01.006.


