


The dermoscopy image of the first case shows a lesion that can be divided into 2 parts (Fig. 1A). On the right side we can see a pattern formed of a central white patch surrounded by a fine pigmented reticulum. This pattern has been reported in 35% to 80% of dermatofibromas and is considered to be the characteristic dermoscopic pattern of such lesions.1 However, on the left side of the image we see a completely different pattern. There are small telangiectasias of short and twisted vessels (kinked vessels) on an erythematous background, and a large arborizing or branching telangiectasia, a structure characteristic of basal cell carcinoma.2 The dermoscopic diagnosis was a collision tumor (dermatofibroma-basal cell carcinoma) and this was confirmed after excision of the lesion.
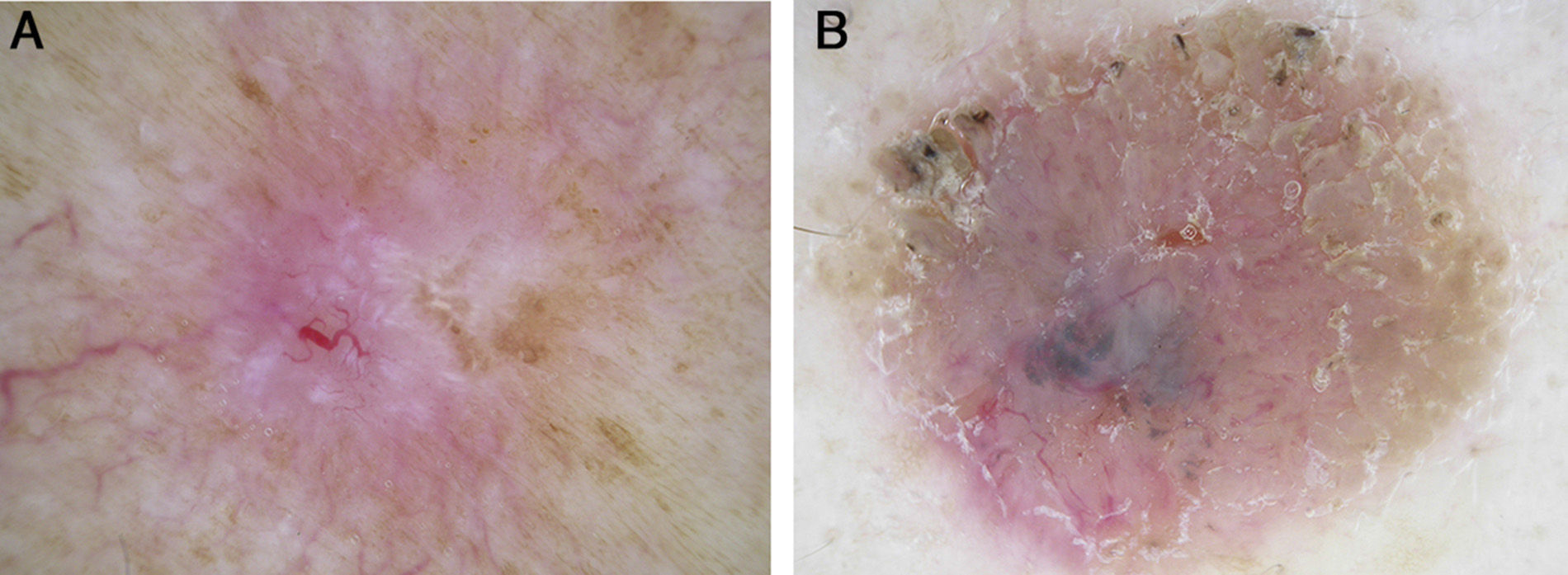
The dermoscopy image of the second case (Fig. 1B) shows fissures and crests, with a few crypts at the periphery of the lesion; these structures are characteristic of seborrheic keratosis.3 However, in the central and lower areas we can see telangiectasias, some of which have an arborizing morphology, ovoid blue-gray areas, and numerous blue-gray globules. These structures are characteristic of basal cell carcinoma.2 The dermoscopic diagnosis was a collision tumor (seborrheic keratosis-basal cell carcinoma) and this was confirmed after excision of the lesion.
The collision of skin tumors is a relatively rare phenomenon (Boyd and Rapini4 found only 69 cases in the 40.000 biopsies they reviewed) and can be difficult to suspect in practice. Diagnostic error is particularly important when the collision tumor is formed of a combination of a malignant and a benign tumor and the benign lesion is clinically more evident, as occurred in both cases presented. By revealing epidermal and dermal structures invisible to the naked eye, dermoscopy has been shown to be very useful in the diagnosis of these lesions, and collision tumors that would normally escape clinical detection can now be diagnosed using this technique (Fig. 2, A and B).5,6
, measuring 1cm in diameter, was different from the other lesions. The clinical diagnosis was inflamed seborrheic keratosis.")
A. An indurated pink nodule of 7×4mm that had been present for years on the left arm of a 67-year-old woman. Positive buttonhole sign. The clinical diagnosis was dermatofibroma. B. Multiple seborrheic keratoses on the back of a 75-year-old man. One of the keratotic papules (center of the photograph), measuring 1cm in diameter, was different from the other lesions. The clinical diagnosis was inflamed seborrheic keratosis.
Please cite this article as: Zaballos-Diego P. Aquí hay «baso» encerrado. Actas Dermosifiliogr. 2014. 105:310–311.


