


There is a need for epidemiological and incidence data on the occurrence of basal cell carcinoma (BCC) in Spain.
ObjectivesOur study was designed to retrospectively retrieve cases from our computer databases from 2010 through 2016 to provide updated data on the actual incidence of BCC in Valencia, eastern Spain.
Material and methodsThis was an epidemiological study on basal cell carcinoma conducted in Valencia, eastern Spain. We analyzed a total of 2171 patients and 4047 tumors, and gathered data to estimate the actual incidence of BBC in our region.
Results and conclusionsOur study confirmed that the incidence of BCC is much higher than previously reported. We calculated a crude incidence of 410.38 BCCs/100 000 person-years, an adjusted rate for the European population of 256.98 BCCs/100 000 person-years, and an adjusted rate for the world population of 196.26 BCCs/100 000 person-years. Risk is up to 29.49% higher for men (464.07 cases/100 000 person-years vs 358.40 cases/100 000 person-years for women). Incidence also increases by an annual 3.91% (a significantly higher annual incidence of 8.28% in women vs a 0.92% annual incidence in men). Overall, the lifetime risk for developing a BCC is 5.8% (5.02% in women and 7% in men).
Existe una necesidad de datos epidemiológicos e incidencia al respecto del carcinoma basocelular (CBC) en España (y en concreto en Valencia).
ObjetivosPara proporcionar datos más actualizados sobre la incidencia real del CBC en Valencia, al este de España, se diseñó un estudio para recuperar casos retrospectivamente de nuestras bases de datos informatizadas entre los años 2010 y 2016.
Material y métodosSe analizaron 2171 pacientes con 4047 CBC de nuestras bases de datos informatizadas, y conjuntamente con los datos poblacionales obtenidos se consiguió hacer una estimación de la incidencia real de este tumor así como su tendencia temporal.
Resultados y conclusionesNuestro estudio confirma que la incidencia del CBC es mucho más alta de lo previamente reportado para nuestra área geográfica. Se calculó una incidencia bruta de 410,38 casos/100.000 hab/año, una incidencia ajustada por población europea de 256,98 casos/100.000 hab/año y una incidencia ajustada por población mundial de 196,26 casos/100.000 hab/año. El riesgo es un 29,49% superior para los hombres (464,07 casos/100.000 hab/año, frente a los 358,40 casos/100.000 hab/año en las mujeres). La incidencia está en aumento a una media del 3,91% por año (significativamente mayor para las mujeres: incrementando un 8,28% al año frente al 0,92% en hombres). El riesgo vital de desarrollar un CBC es del 5,8% globalmente, siendo del 5,02% para las mujeres y del 7% para los hombres.

Basal cell carcinoma (BCC) is the most common malignant neoplasm in humans, both among dermatological conditions and globally. It originates at the basal layer of the epidermis and appendages, which has an impact on its progression and clinical signs.
Although it is a tumor with a high incidence rate, elevated cure rate, and multiple therapeutic options, systematic records are scarce, making high-quality epidemiological studies challenging.
Former epidemiological studies conducted worldwide have found extremely variable incidences, ranging from < 1 case per 100,000 inhabitants per year in Kenya 1 to > 1500 cases per 100,000 inhabitants per year in Australia.2
In Spain, the incidence rate seems to be at an intermediate level, around 250 cases per 100,000 inhabitants per year.
There are few extensive studies on this topic in the literature, primarily 2 patient registries, one from Soria (1998 to 2000) 3 and the other one from Girona (1994 to 2007, later extended to 2012),4 which lack data on individual tumors and second tumors (a relevant issue, as synchronous and metachronic tumor multiplicity of BCC has been demonstrated).5 Both studies reported a crude incidence rate of nearly 150 cases per 100,000 inhabitants per year.
In a different study—methodologically more correct but covering only 1 year6 —in the Barcelonés region, all BCC diagnoses were collected, yielding a more accurate estimate of 253.2 cases per 100,000 inhabitants per year.
It has been reported in studies worldwide—including the previously mentioned Girona study7 —that the incidence rate of BCC is on the rise.
We conducted this retrospective study to provide updated and as accurate data as possible on the incidence of BCC in our region (Valencia).
Materials and methodsOur study population was assigned to the Department of Hospital Universitario Dr. Peset in Valencia, which covers approximately 20% of the population of Valencia and its metropolitan area (about 345,000 people).
The study design was submitted and approved by our hospital Ethics and Clinical Research Committee (June 30th, 2017, CEIC Code: 76/17).
Using the data extraction tools of computerized health records, we filtered all patients diagnosed with suspected basal cell carcinoma—including those from other specialties—treated in our health department (both in hospital consultations and in the outpatient specialty center affiliated with the same department and sharing the assigned population) from 2010 through 2016.
This time frame was selected because it included complete years when it was possible to analyze the health records when the project was presented to the CEIC.
This search yielded more than 30,000 entries of health records from a total of 7425 patients. Complete records of 3057 of these patients were reviewed and randomly selected due to the immense volume of data (41.17%) to find 2171 patients with a confirmed diagnosis. With this sample, the total number of patients is estimated at 5273.
Both histological and clinical-dermoscopic diagnoses were accepted as confirmed for dermatology records when no alternative diagnosis was present (15.59% of cases). This clinical criterion—although different from the exclusively histological approach used in other studies—is more representative of reality, as it has been demonstrated that, assisted by dermoscopy, dermatologists yield a diagnostic accuracy > 98% for this type of tumor.8
After reviewing the records, a total of 4047 BCCs were found during the study period, averaging 1.86 BCCs per person (with an estimated 9830 in the entire sample).
For sex analysis, according to current recommendations, the sex assigned at birth (based on external anatomy and chromosomal genotype) was considered the defining factor.
Accurate and updated population data from our health department were collected annually from the Valencian Institute of Statistics (IVE).9Table 1 shows a significant variation in the population covered by our department starting in 2015 due to a reorganization of areas conducted at the end of the previous year.
Incidence rates of basal cell carcinoma and trends.
| Year | Population | BCC in sample | BCC in population (estimate) | Incidence (BCC/100,000 inhabitants per year) | Variation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women | Men | Total | Women | Men | Total | Women | Men | Total | Women | Men | Total | Women | Men | Total | |
| 2010 | 192,672 | 186,553 | 379,225 | 224 | 327 | 551 | 544.06 | 794.23 | 1338.30 | 282.38 | 425.74 | 352.90 | - | - | - |
| 2011 | 193,194 | 187,058 | 380,252 | 249 | 360 | 609 | 604.78 | 874.39 | 1479.17 | 313.05 | 467.44 | 389.00 | +10.86 | +9.79 | +10.23 |
| 2012 | 188,259 | 182,281 | 370,540 | 218 | 344 | 562 | 529.49 | 835.53 | 1365.01 | 281.26 | 458.37 | 368.39 | −10.15 | −1.94 | −5.30 |
| 2013 | 187,712 | 181,750 | 369,462 | 297 | 324 | 621 | 721.37 | 786.95 | 1508.32 | 384.30 | 432.98 | 408.25 | +36.64 | −5.54 | +10.82 |
| 2014 | 185,088 | 179,211 | 364,299 | 294 | 376 | 670 | 714.08 | 913.25 | 1627.33 | 385.81 | 509.59 | 446.70 | +0.39 | +17.69 | +9.42 |
| 2015 | 141,005 | 136,528 | 277,533 | 255 | 284 | 539 | 619.36 | 689.79 | 1309.15 | 439.24 | 505.24 | 471.71 | +13.85 | −0.85 | +5.60 |
| 2016 | 140,188 | 135,736 | 275,924 | 244 | 251 | 495 | 592.64 | 609.64 | 1202.28 | 422.75 | 449.14 | 435.73 | −3.76 | −11.1 | −7.63 |
| Average | 175,445 | 169,873 | 345,319 | 254.43 | 323.71 | 578.14 | 617.97 | 786.25 | 1404.22 | 358.40 | 464.07 | 410.38 | +8.28 | +0.92 | +3.91 |
The characteristics of the population covered by our health department (in terms of age distribution, income, and other factors) are very similar to those of other departments in the Valencia metropolitan area, according to data provided by IVE, so it is reasonable to assume that the distribution is sufficiently homogeneous for the results to be applicable to the entire geographic area.
ResultsKnowing the estimated cases (quite precisely due to our high n) in our study area, the population assigned to our health department (which varies from year to year), and age distribution (which was practically constant throughout the period), we can calculate the crude incidence rate of basal cell carcinoma, the age-specific incidence rate, and the annual variation in incidence. All these data are collected in Table 1 1.
During the studied period, the mean crude incidence rate is 410.38 cases per 100,000 inhabitants per year, which is significantly higher than previously reported figures.
When analyzing by sex, the incidence in men is up to 29.49% higher, reaching 464.07 cases per 100,000 inhabitants per year, while for women it is only 358.40 cases per 100,000 inhabitants per year.
Moreover, the trend towards increasing incidence is clear, with a variation between the first and the last (7th) year of the study of 23.47%, and a mean annual increase estimated at 3.91%.
This increase is especially pronounced in women, with an annual rise of 8.28% vs only 0.92% in men.
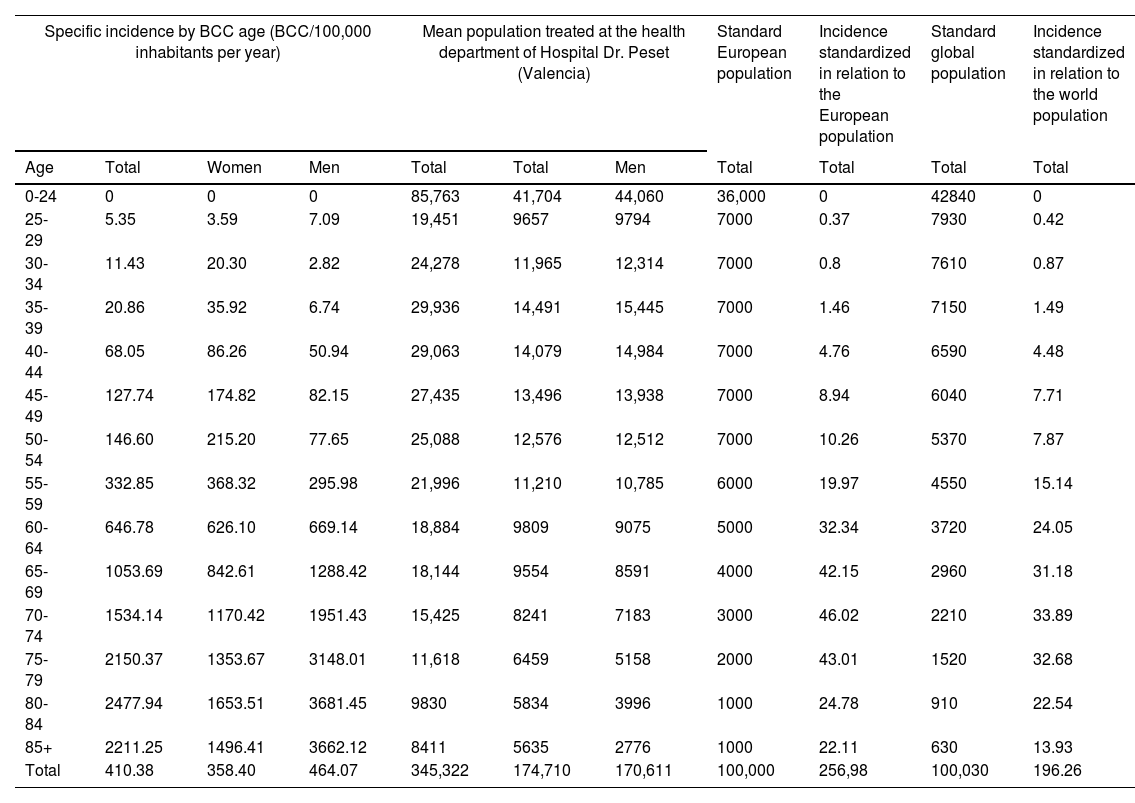
To enhance the comparability of our results, mean population values for each age range were collected, as well as the incidence (also calculated separately by sex) and included in the corresponding table (Table 2) to standardize our rates with the European population 10: 256.98 cases per 100,000 inhabitants per year; and with the global population 11: 196.26 cases per 100,000 inhabitants per year.
Age-specific incidence by sex, standardized to European and global populations.
| Specific incidence by BCC age (BCC/100,000 inhabitants per year) | Mean population treated at the health department of Hospital Dr. Peset (Valencia) | Standard European population | Incidence standardized in relation to the European population | Standard global population | Incidence standardized in relation to the world population | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | Total | Women | Men | Total | Total | Men | Total | Total | Total | Total |
| 0-24 | 0 | 0 | 0 | 85,763 | 41,704 | 44,060 | 36,000 | 0 | 42840 | 0 |
| 25-29 | 5.35 | 3.59 | 7.09 | 19,451 | 9657 | 9794 | 7000 | 0.37 | 7930 | 0.42 |
| 30-34 | 11.43 | 20.30 | 2.82 | 24,278 | 11,965 | 12,314 | 7000 | 0.8 | 7610 | 0.87 |
| 35-39 | 20.86 | 35.92 | 6.74 | 29,936 | 14,491 | 15,445 | 7000 | 1.46 | 7150 | 1.49 |
| 40-44 | 68.05 | 86.26 | 50.94 | 29,063 | 14,079 | 14,984 | 7000 | 4.76 | 6590 | 4.48 |
| 45-49 | 127.74 | 174.82 | 82.15 | 27,435 | 13,496 | 13,938 | 7000 | 8.94 | 6040 | 7.71 |
| 50-54 | 146.60 | 215.20 | 77.65 | 25,088 | 12,576 | 12,512 | 7000 | 10.26 | 5370 | 7.87 |
| 55-59 | 332.85 | 368.32 | 295.98 | 21,996 | 11,210 | 10,785 | 6000 | 19.97 | 4550 | 15.14 |
| 60-64 | 646.78 | 626.10 | 669.14 | 18,884 | 9809 | 9075 | 5000 | 32.34 | 3720 | 24.05 |
| 65-69 | 1053.69 | 842.61 | 1288.42 | 18,144 | 9554 | 8591 | 4000 | 42.15 | 2960 | 31.18 |
| 70-74 | 1534.14 | 1170.42 | 1951.43 | 15,425 | 8241 | 7183 | 3000 | 46.02 | 2210 | 33.89 |
| 75-79 | 2150.37 | 1353.67 | 3148.01 | 11,618 | 6459 | 5158 | 2000 | 43.01 | 1520 | 32.68 |
| 80-84 | 2477.94 | 1653.51 | 3681.45 | 9830 | 5834 | 3996 | 1000 | 24.78 | 910 | 22.54 |
| 85+ | 2211.25 | 1496.41 | 3662.12 | 8411 | 5635 | 2776 | 1000 | 22.11 | 630 | 13.93 |
| Total | 410.38 | 358.40 | 464.07 | 345,322 | 174,710 | 170,611 | 100,000 | 256,98 | 100,030 | 196.26 |
As seen in the age-specific incidence columns in Table 2, the risk of developing a BCC is higher for women up to age 60. After that, the risk in men increases significantly, doubling that of women from age 75 onwards.
According to our data, up to 42% of patients will have, at least, a second BCC. Overall, the mean count is 1.86 BCCs per patient, higher for men (2.13 BCCs/patient) vs women (1.6 BCCs/patient).
With the previous incidence estimates across all age ranges and the mentioned data on tumor multiplicity in a single patient, the lifetime risk of developing a BCC for our geographic area can also be estimated. Overall, the risk is 5.8% (5.02% for women and 7% for men).
DiscussionWe present an epidemiological study based on the retrospective review of health records from a health department in Valencia—both hospital and outpatient—to provide the most accurate approximation possible to the real incidence of basal cell carcinoma.
Although the study period (2010-2016) may seem distant from the present time, it is up-to-date compared to other Spanish studies,3,4,6,7 and, as far as we know, it is the first one focused on Valencia and its metropolitan area.
The results obtained show a higher incidence than previously reported in other Spanish studies, and this incidence is clearly increasing.
Furthermore, the excess risk for men is similar to the 26% reported in former studies 4, being closer to the 30% observed in our results.
Overall, our findings on the upward trend in incidence are consistent with other global studies—including Spanish studies—around a 6% annual increase, with a greater rise for women. Our data show more pronounced differences in trends by sex vs most previous studies.12
Since the incidence has been standardized to the European and global populations, a more realistic comparison with other regions and countries in our environment and worldwide can be made, positioning us at an intermediate point between countries with extreme risk, such as Australia, and those with low risk, such as Central African countries.
Additionally, the data obtained have allowed the calculation for the first time—something never done in the previously mentioned studies—of the lifetime risk (around 6%) of developing a BCC in a Spanish population.
Although having more up-to-date data would undoubtedly be optimal, the above-mentioned lack of specific records requires a thorough review of health records, a process that is time-consuming and delays results. It would be of great epidemiological interest to obtain successive data from our area in subsequent years and examine the variation during and after the COVID-19 pandemic.
On the other hand, our study has some limitations:
As stated, BCC cases without histological confirmation were accepted, so our incidence will be more realistic but inevitably higher than studies based solely on histological diagnoses.
Patient mobility between health departments, although likely balanced in its flows, prevents a completely precise estimate of the study population.
Similarly, it is impossible to quantify how many patients from our area are diagnosed and treated in private medicine, as we have no records on this topic. Some studies 13 suggest that up to 18.5% of malignant keratinocytic neoplasms—without differentiating among BCC, squamous cell carcinoma, and others—receive care outside the public system, which means that we might be underestimating this non-negligibly.
While the interannual variability of incidence—especially when broken down by sex—is noteworthy, the upward trend is unequivocal given the data over 7 consecutive years.
Finally, there is no comparative data with other regions of Spain in terms of phototypes, solar exposure, ethnicity, and other risk factors, so our conclusions might not be applicable to the entire national territory.
ConclusionsIn conclusion, our study confirms that the incidence of basal cell carcinoma in the studied population is much higher than previously reported in other regions of Spain, thus providing more specific data—not previously available—for our geographic area (Valencia). We have managed to estimate the lifetime risk of developing this tumor.
Moreover, by demonstrating an increasing incidence, the importance of conducting new epidemiological studies to update our knowledge and provide a more accurate perspective on the disease seems obvious.
FundingNone declared.
Conflicts of interestNone declared.


