





Hidradenitis suppurativa (HS) is a chronic, progressive inflammatory disease with a substantial impact on quality of life. Accessibility to specialized units and referral methods may significantly influence clinical characteristics and therapeutic decisions. This study aims to analyze the relationship between geographical distance, referral method, and the clinical and therapeutic characteristics of patients with HS.
Materials and methodsThis was a cross-sectional study including 557 consecutive patients treated between 2017 and 2024 at the HS Unit of Hospital Universitario Virgen de las Nieves. Clinical, demographic, and treatment-related variables were collected. Geographical distance was calculated based on postal codes, and differences between referral methods (teledermatology vs conventional) were analyzed using descriptive and comparative statistical methods.
ResultsPatients residing at greater distances presented with more severe disease (Hurley stage III, higher IHS4 scores) and poorer quality of life (DLQI). They also required more intensive treatment regimens, with increased use of biological immunomodulatory drugs. Patients referred via teledermatology were generally younger, had a shorter disease duration, and exhibited milder disease severity at the time of consultation.
ConclusionsGeographical distance and referral method may significantly influence the clinical and therapeutic profiles of patients with HS. These findings underscore the need for strategies to improve accessibility and ensure equitable management. Teledermatology emerges as a valuable tool for early-stage cases, although it should be complemented with in-person assessments for more complex cases.

Hidradenitis suppurativa (HS) is a chronic inflammatory disease affecting the hair follicle, predominantly involving intertriginous areas such as the axillae and the inguinogenital region. The prevalence of HS varies considerably and is estimated at approximately 1% of the general population. Diagnosis is often substantially delayed, with an average delay ranging from 7.2 to 10.2 years, which has important clinical implications.1,2 This delay prevents the initiation of early treatment during the so-called “window of opportunity,” a critical period in which intervention may prevent progression to irreversible structural skin damage.3,4
The diagnosis of HS is based on well-established clinical criteria, including the presence of recurrent lesions in typical anatomical areas for at least 6 months.5 To complement the diagnosis, several standardized and validated scoring systems have been developed, such as the Hurley Staging System and the International Hidradenitis Suppurativa Severity Score System (IHS4), which allow assessment of structural disease severity and inflammatory burden, respectively.6 These tools are essential not only for standardizing patient evaluation in clinical and epidemiological studies, but also for guiding therapeutic decisions and monitoring treatment response.5
The management of HS is particularly complex and requires a multidisciplinary approach, including a combination of medical therapies, such as retinoids, topical and systemic antibiotics, and immunomodulators, along with interventional and surgical procedures.4 Despite therapeutic advances, the disease course remains variable and often unpredictable. Some patients exhibit a relatively stable course, whereas others develop early and progressive structural damage.7 Therefore, ensuring early access to specialized HS units is essential. These units not only facilitate a faster and more accurate diagnosis, but also enable the implementation of personalized therapeutic strategies that optimize comprehensive disease management and improve patient prognosis.4,8
The objectives of this study were (a) to analyze the influence of geographic distance from patients’ place of origin on their clinical characteristics and on therapeutic decisions made during the first visit to the Hidradenitis Suppurativa Unit of Hospital Virgen de las Nieves (Granada, Spain), and (b) to explore the relationship between clinical characteristics and therapeutic decisions according to the referral method, either via teledermatology or conventional referral.
Materials and methodsThe Materials and Methods section is described in detail in the Appendices (Appendix 5.1, Materials and Methods).
ResultsGeneral characteristics of the study populationThe cohort included a total of 557 patients diagnosed with hidradenitis suppurativa. Sex distribution was balanced, with 49.19% men (n=274) and 50.81% women (n=283). The mean age was 41.87 years (SD, 14.19). A total of 58.17% of patients were smokers (n=324), and the mean body mass index (BMI) was 29.64 (SD, 6.89). Family history of the disease was reported in 40.93% of patients (n=228). The mean disease duration was 17.52 years (SD, 11.5), and the mean age at disease onset was 24.34 years (SD, 12.35). According to the Hurley classification, 37.16% (n=207) were classified as stage I, 46.49% (n=259) as stage II, and 16.34% (n=91) as stage III (Appendices, Table A.1).
At the index visit to the HS unit, patients exhibited a mean of 1.05 abscesses (SD, 1.75) and 1.17 inflammatory or draining tunnels (SD, 1.86). The mean IHS4 score was 8.45 (SD, 9.11), and the mean number of affected areas was 1.83 (SD, 1.03). Regarding therapeutic decisions, 9.69% of patients (n=54) had previously received biologic therapy for HS, whereas 15.44% (n=86) were prescribed biologic treatment during the index to the HS unit. In addition, 10.05% of patients (n=56) were considered candidates for dermatologic surgery (Appendices, Table A.1).
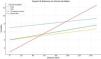
Clinical characteristics and therapeutic decisions according to geographic distance (road distance in kilometers) from patients’ place of origin to Hospital Universitario Virgen de las NievesPatients living farther away showed a higher proportion of advanced Hurley stage III disease (β coefficient=77; SD, 6.6; P<.0001). Similarly, the number of affected areas (β=10.69; SD, 2.63; P<.0001), the number of inflammatory or draining tunnels (β=9.23; SD, 1.43; P<.0001), and scores on the visual analog scales (VAS) for pain (β=2.41; SD, 0.96; P=.012), malodor (β=2.20; SD, 0.76; P=.004), suppuration (β=1.79; SD, 0.79; P=.024), pruritus (β=1.82; SD, 0.79; P=.021), and overall VAS (β=2.45; SD, 0.96; P=.011) were significantly higher among patients living farther from the hospital (Table 1; Fig. 1).
Clinical characteristics and therapeutic decisions according to geographic distance in road kilometers of patients with HS (N=557).
| Variables | Geographic distance in road kilometers | p value |
|---|---|---|
| Age (years)a | −0.25 (SD, 0.19) | 0.19 |
| Sexb | ||
| Male | 45.92 (SD, 3.93) | 0.12 |
| Female | 54.47 (SD, 3.88) | |
| Smokingb | ||
| Yes | 50 (SD, 3.62) | 0.91 |
| No | 50.64 (SD, 4.26) | |
| Disease duration (years)a | 0.2 (SD, 0.24) | 0.39 |
| Age at onset (years)a | −0.51 (SD, 0.22) | 0.02 |
| Martorell phenotypeb | 0.21 | |
| Follicular: 37.14 (SD, 9.38) | ||
| Inflammatory: 50.62 (SD, 3.01) | ||
| Mixed: 60.88 (SD, 9.8) | ||
| Hurley stageb | <0.0001 | |
| Hurley I: 35.41 (SD, 4.43) | ||
| Hurley II: 52.7 (SD, 3.9) | ||
| Hurley III: 77 (SD, 6.6) | ||
| Pilonidal sinusb | 59.17 (SD, 4.88) | 0.028 |
| Number of affected areasa | 10.69 (SD, 2.63) | <0.0001 |
| Inflammatory nodulesa | 0.86 (SD, 2.24) | 0.44 |
| Abscessesa | 0.65 (SD, 1.58) | 0.68 |
| Inflammatory or draining tunnelsa | 9.23 (SD, 1.43) | <0.0001 |
| Pain VAS 0–10a | 2.41 (SD, 0.96) | 0.012 |
| Malodor VAS 0–10a | 2.20 (SD, 0.76) | 0.004 |
| Drainage VAS 0–10a | 1.79 (SD, 0.79) | 0.024 |
| Pruritus VAS 0–10a | 1.82 (SD, 0.79) | 0.021 |
| Global VAS 0–10a | 2.45 (SD, 0.96) | 0.011 |
| IHS4a | 1.83 (SD, 0.29) | <0.0001 |
| DLQIa | 1.55 (SD, 0.38) | <0.0001 |
| Therapeutic burdena | 7.74 (SD, 1.18) | <0.0001 |
| Prior biologic treatmentb | 46.19 (SD, 2.85) | <0.0001 |
| Prescription of biologic treatmentb | <0.0001 | |
| Yes | 90.68 (SD, 6.76) | |
| No | 42.87 (SD, 2.89) | |
| Indication for dermatologic surgeryb | 70.48 (SD, 8.65) | 0.014 |
HS, hidradenitis suppurativa; SD, standard deviation; BMI, body mass index; IBD, inflammatory bowel disease; IHS4, International Hidradenitis Suppurativa Severity Score System; DLQI, Dermatology Life Quality Index.
Values in bold indicate p<0.05.

Furthermore, DLQI (β=1.55; SD, 0.38; P<.0001), IHS4 (β=1.83; SD, 0.29; P<.0001), and therapeutic burden (β=7.74; SD, 1.18; P<.0001) increased significantly with distance. Patients living farther away were more likely to have received prior biologic treatments (β=46.19; SD, 2.85; P<.0001), to be prescribed biologic therapy (β=90.68; SD, 6.76; P<.0001), or to be referred for dermatologic surgery (β=70.48; SD, 8.65; P=.014) at the index visit to the HS unit (Table 1; Fig. 1).
Comparison according to province of origin of patients with HSPatients residing outside the province of Granada (Spain) (n=139) showed significant differences vs those living in Granada (n=418). The former had a longer disease duration (19.28 vs 16.94 years; P=.037), an earlier age at onset (22.43 vs 24.98 years; P=.034), and a greater number of affected areas (2.20 vs 1.71; P<.0001). Furthermore, they showed a higher prevalence of pilonidal sinus (41.73% vs 28.23%; P=.003), a higher proportion of Hurley stage III disease (32.37% vs 11.00%; P<.0001), and higher IHS4 (13.43 vs 6.80; P<.0001), DLQI (12.77 vs 9.72; P<.0001), and overall VAS scores (5.28 vs 4.56; P=.009) (Appendices, Table A.2).
Regarding therapeutic decisions, patients from outside Granada more frequently had prior biologic therapy (21.58% vs 5.74%; P<.0001), were prescribed biologic treatment (33.81% vs 9.33%; P<.0001), and were referred for dermatologic surgery (15.11% vs 8.37%; P=.022) at the first visit to the HS unit (Appendices, Table A.2).
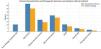
Comparison according to referral method to the HS unit at Hospital Universitario Virgen de las NievesSignificant differences were observed between patients referred via teledermatology (n=47) and those referred through the conventional pathway (n=510). Patients referred vis teledermatology were younger (35.25 vs 42.48 years; P<.001), had a shorter disease duration (14.06 vs 17.84 years; P=.031), and an earlier age at onset (21.19 vs 24.63 years; P=.033). Moreover, these patients showed lower scores for VAS pain (3.53 vs 4.86; P=.002), overall VAS (3.51 vs 4.85; P=.002), DLQI (7.78 vs 10.73; P=.006), and IHS4 (6.87 vs 8.60; P=.213). In addition, teledermatology-referred patients had a lower therapeutic burden (1.32 vs 2.52; P<.001) and no past medical history of prior biologic therapy (0% vs 10.59%; P=.019) (Table 2; Fig. 2).
Clinical characteristics and therapeutic decisions according to referral method to the HS Unit of Hospital Universitario Virgen de las Nieves (N=557).
| Referral method | Conventional referral(N=510) | Teledermatology(N=47) | p value |
|---|---|---|---|
| Age (years) | 42.48 (SD, 0.62) | 35.25 (SD, 2.05) | <0.001 |
| Sex (male/female) | 49.61% (253/510)/50.39% (257/510) | 44.68% (21/47)/55.32% (26/47) | 0.418 |
| Smoking | 58.04% (296/510) | 59.57% (28/47) | 0.838 |
| BMI | 29.59 (SD, 0.30) | 30.10 (SD, 1.00) | 0.629 |
| Disease duration (years) | 17.84 (SD, 0.50) | 14.06 (SD, 1.67) | 0.031 |
| Age at onset (years) | 24.63 (SD, 0.54) | 21.19 (SD, 1.79) | 0.033 |
| Martorell phenotype | <0.0001 | ||
| Follicular: 7.84% (40/510) | Follicular: 19.15% (9/47) | ||
| Inflammatory: 85.49% (436/510) | Inflammatory: 59.57% (28/47) | ||
| Mixed: 6.67% (34/510) | Mixed: 21.28% (10/47) | ||
| Hurley stage | 0.289 | ||
| Hurley I: 36.27% (185/510) | Hurley I: 46.81% (22/47) | ||
| Hurley II: 46.86% (239/510) | Hurley II: 42.55% (20/47) | ||
| Hurley III: 16.87% (86/510) | Hurley III: 10.64% (5/47) | ||
| Pilonidal sinus | 30.98% (158/510) | 38.30% (18/47) | 0.301 |
| Number of affected areas | 1.82 (SD, 0.04) | 1.93 (SD, 0.15) | 0.467 |
| Inflammatory nodules | 1.60 (SD, 0.18) | 2.23 (SD, 0.60) | 0.305 |
| Abscesses | 1.09 (SD, 0.07) | 0.61 (SD, 0.25) | 0.072 |
| Inflammatory or draining tunnels | 1.20 (SD, 0.08) | 0.85 (SD, 0.27) | 0.214 |
| Pain VAS 0–10 | 4.86 (SD, 0.12) | 3.53 (SD, 0.41) | 0.002 |
| Global VAS 0–10 | 4.85 (SD, 0.12) | 3.51 (SD, 0.41) | 0.002 |
| IHS4 | 8.60 (SD, 0.40) | 6.87 (SD, 1.32) | 0.213 |
| DLQI | 10.73 (SD, 0.31) | 7.78 (SD, 1.03) | 0.006 |
| Therapeutic burden | 2.52 (SD, 0.09) | 1.32 (SD, 0.32) | <0.001 |
| Prior biologic treatment | 10.59% (54/510) | 0% (0/47) | 0.019 |
| Prescription of biologic treatment | 16.27% (83/510) | 6.38% (3/47) | 0.072 |
| Indication for dermatologic surgery | 10.39% (53/510) | 6.38% (3/47) | 0.381 |
HS, hidradenitis suppurativa; SD, standard deviation; BMI, body mass index; VAS, Visual Analog Scale; IHS4, International Hidradenitis Suppurativa Severity Score System; DLQI, Dermatology Life Quality Index. Continuous data are expressed as mean (SD) and categorical data as % (proportion). Values in bold indicate p<0.05.

This study provides evidence on the potential influence of geographic distance and referral method on the clinical characteristics and therapeutic decisions of patients with HS. Our findings suggest the importance of adopting strategies to improve accessibility to specialized units, highlighting the impact that such accessibility has on the comprehensive management of this complex disease.9
Regarding geographic distance and province of origin, patients from more distant areas showed a more severe clinical profile, characterized by a higher proportion of advanced Hurley stages, a greater number of inflammatory or draining tunnels and affected areas, as well as worse scores on quality-of-life indices and visual analog scales. These results are consistent with former studies suggesting that geographic barriers may delay access to specialized care, resulting in delayed diagnosis and treatment.10,11 In addition, patients living farther away had a higher therapeutic burden and were more likely to require biologic therapies or dermatologic surgery, underscoring the importance of early accessibility to prevent disease progression and improve prognosis. The increased proportion of patients from distant areas treated with biologic drugs may be explained by greater disease severity and the need for advanced therapeutic options.4
With respect to the referral method to the HS unit, patients referred via teledermatology exhibited milder clinical characteristics compared with those referred via conventional pathways. These patients were younger, had a shorter disease duration, and lower scores on severity scales such as the DLQI and VAS. These findings suggest that teledermatology may facilitate earlier detection of less severe cases, allowing timely intervention before disease progression. Moreover, teledermatology-referred patients showed a lower therapeutic burden and no prior biologic treatments, indicating that this referral method may be particularly useful for identifying patients in the early stages of the disease.
Early care in HS is essential to prevent disease progression, given its progressive and irreversible nature. This approach is comparable to the protocolized management of critical conditions such as stroke and myocardial infarction, in which immediate care is vital to minimize tissue damage. In stroke, for example, reperfusion therapies administered within the first few hours have been shown to significantly reduce long-term disability.12 Similarly, in myocardial infarction, timely primary angioplasty is associated with lower mortality and improved cardiac function.13 In dermatology, this principle of early detection and intervention is evident in melanoma management, where early diagnosis increases survival rates and allows less invasive interventions.14 These comparisons highlight the need to implement systems that prioritize early care for patients with hidradenitis suppurativa. Ensuring early access to specialized units is essential to achieve accurate and timely diagnoses and to establish effective therapeutic strategies capable of halting disease progression and reducing long-term complications. This approach not only optimizes comprehensive patient management but also helps minimize the physical and psychosocial impact of the disease.11
Our findings are consistent with international studies highlighting the clinical heterogeneity of HS and the influence of sociodemographic factors on its management.15,16 Recent studies have emphasized the importance of addressing geographic and economic inequalities to improve outcomes in patients with HS.11,17 In addition, the usefulness of teledermatology as a tool to improve accessibility and early detection has been previously documented,18–20 although our study is among the few to specifically evaluate its impact on HS.
One of the main strengths of our study is the inclusion of a large and representative cohort, allowing for an in-depth analysis of the impact of geographic and referral-related factors on clinical characteristics and therapeutic decisions. Furthermore, the use of validated tools to assess disease severity, such as IHS4, Hurley stages, and DLQI, reinforces the robustness of the data obtained.
Nevertheless, the cross-sectional design of the study limits the ability to establish causal relationships. In addition, the smaller sample size of the teledermatology-referred group (n=47) vs the conventionally referred group (n=510) introduces an asymmetry that may limit statistical power to detect subtle differences between groups and may affect the generalizability of these findings.
Finally, although our results are applicable to the context of a specialized unit, their generalization to other settings may be limited due to differences in health care organization and available resources.
In conclusion, this study highlights the potential influence of geographic distance and referral method on the clinical characteristics and therapeutic decisions of patients with HS. Patients living farther away present with greater clinical severity and require more advanced therapeutic strategies, underscoring the need to ensure equitable access to specialized units and to promote the development of additional specialized centers within hospitals. On the other hand, teledermatology emerges as a valuable tool for early case detection with the aim of reducing therapeutic delay.
Overall, our findings reinforce the importance of adopting multidisciplinary strategies that address geographic barriers and optimize patient referral pathways to improve clinical outcomes and quality of life for patients with HS. Future longitudinal studies will be necessary to confirm our observations and to evaluate the impact of specific interventions on HS patient care.
Conflict of interestThe authors declare that they have no conflict of interest.
The followings are the supplementary data to this article:



