





Darier disease (DD) is an uncommon autosomal dominant genodermatosis caused by mutations of the ATP2A2 gene, which encodes the sarcoplasmic/endoplasmic reticulum calcium-ATPase isoform 2 (SERCA2). Disfunction of this pump disturbs intracellular Ca2+ signaling, compromising keratinocyte differentiation and intercellular adhesion.1 Although many therapeutic modalities have been investigated, treatment of DD remains challenging, as their efficacy is often unsatisfactory. We describe two cases of DD efficiently treated with oral retinoids in association with topical diclofenac sodium 3% gel.
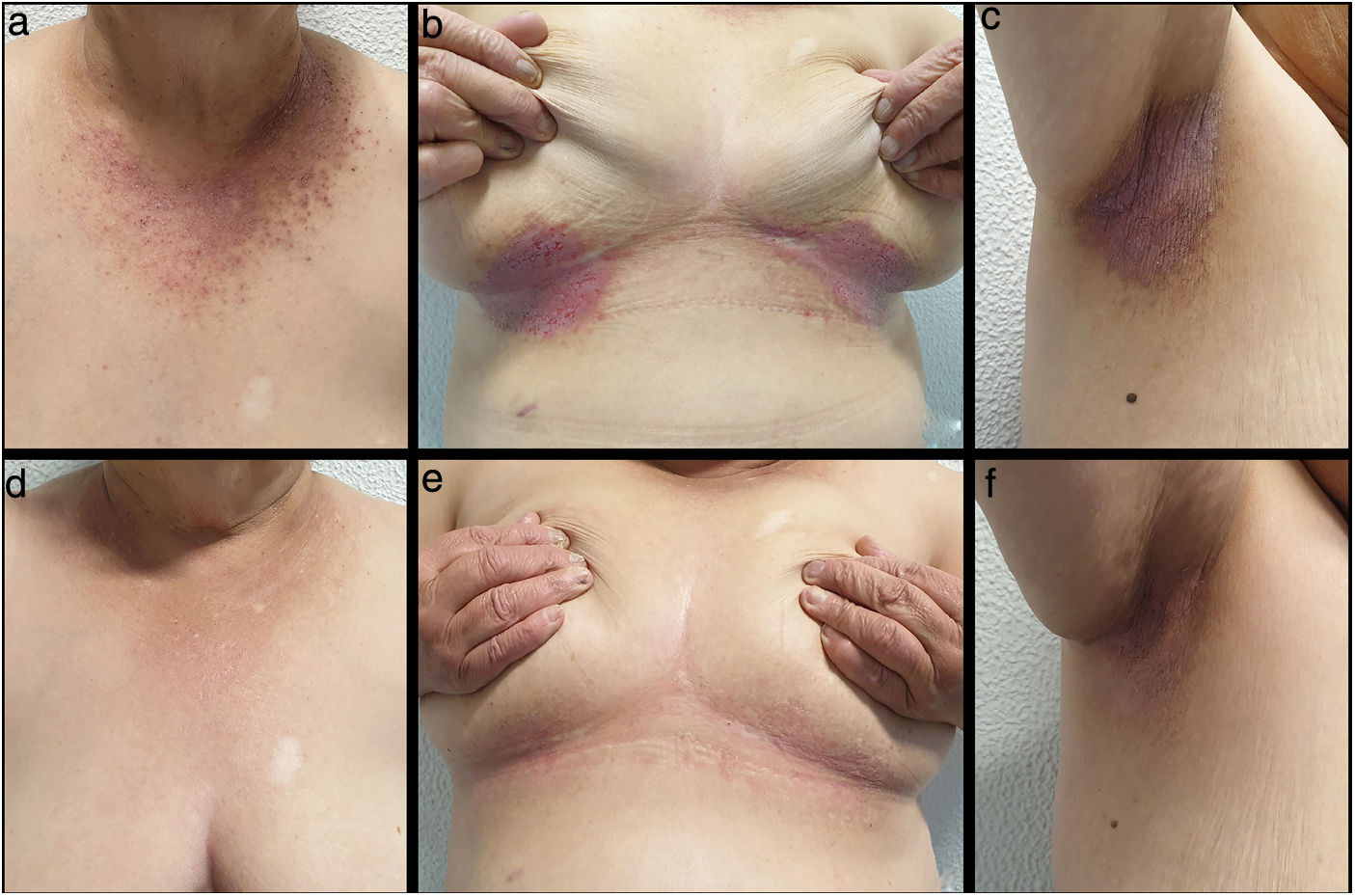
Patient 1 was a 68-year-old woman, with DD diagnosed at 20 years of age, who presented with multiple hyperkeratotic papules on her neck, trunk and back and moisty, fissured plaques on her axillae, submammary folds and groin. She had been treated with topical therapies, including steroids, retinoids, calcineurin inhibitors and urea cream, with unsatisfactory control. During an extensive exacerbation, acitretin 25mg treatment was started with mild improvement after three months. Recalcitrant disease led us to combine acitretin with topical diclofenac sodium 3% gel, which was applied twice daily. There was a dramatic improvement in the first two weeks, and complete remission was obtained after a further 8 weeks (Fig. 1). The patient remained asymptomatic for the following six months. As maintenance therapy, diclofenac sodium 3% gel application was reduced to once a day without relapse during a six-month follow-up period.
Patient 2 was a 41-year-old woman, daughter of patient 1, who suffered from therapy-resistant DD for 23 years. She presented with numerous coalescent hyperkeratotic papules on her trunk. Conventional topical treatments were not successful and isotretinoin 30mg once daily only during three months resulted in slight improvement. Based on the satisfying response observed in her mother, diclofenac sodium 3% gel was started twice daily, in association with isotretinoin. There was a significant improvement after 12 weeks and the patient remained well-controlled for the following 9 months without noticeable side effects (Fig. 2).

Diclofenac sodium is a nonsteroidal anti-inflammatory drug (NSAID) that suppresses inflammation by inhibiting the activity of cyclooxygenase enzymes (COX-1 and COX-2). Kamijo et al. supported the role of COX-2 in the pathogenesis of DD by showing that its expression induced by ultraviolet B (UVB) reduces both ATP2A2 gene expression and SERCA2 production in keratinocytes. Furthermore, COX-2 inhibition was shown to increase ATP2A2 mRNA expression and SERCA2 levels both in ultraviolet (UV)-irradiated and non-UV-irradiated normal human keratinocytes.2,3
Recently, four cases of successful treatment of DD with diclofenac sodium 3% gel and one case with diclofenac sodium 1% gel have been reported.4–7 To the best of our knowledge, this is the first report of successful combination of this therapy with oral retinoids.
In both patients, diclofenac sodium seemed to potentiate the improvement observed with oral retinoid treatment. Indeed, diclofenac sodium and retinoids may share a mechanism of action and present synergic effects, as retinoids also suppress COX-2 production.8
To date, no reports of successful treatment of DD with oral NSAIDs have been published. Nevertheless, topical administration is a more attractive route, as it can achieve high skin concentrations and avoid potential systemic side effects.
In conclusion, the combination of oral retinoids and diclofenac sodium 3% gel could be an effective and safe alternative for DD patients who do not respond to or are intolerant to conventional treatments.


