



A 76-year-old man with a history of hypertension, dyslipidemia, and cerebral vascular accident presented with a necrotic lesion and intense inflammation of the surrounding soft tissues on the left forearm. He attributed the lesion to a sting or bite of unknown origin during a hunting outing in the month of July. The ulcer worsened despite treatment with oral doxycycline and intravenous amoxicillin-clavulanic acid, and the patient was administered intravenous broad-spectrum empiric antibiotic therapy with imipenem and amphotericin B (Fig. 1). Hematoxylin-eosin staining of a biopsy specimen showed branching hyphae in the subcutaneous tissue together with necrosis and an intense inflammatory infiltrate. Cultures were negative for aerobic and anaerobic bacteria and mycobacteria. Fungal culture in Sabouraud-dextrose agar permitted the identification of the microorganism responsible for the infection after 48hours incubation at 30°C. Microscopic examination with lactophenol cotton blue revealed the growth of a white downy colony, without sporulation, in addition to typical wide, aseptate hyphae with right-angle branching characteristic of Mucorales fungi. The strain was sent to the Mycology Laboratory at Instituto de Salud Carlos III, where it was identified as Saksenaea vasiformis with a minimum inhibitory concentration of 2μg/mL for amphotericin B, >8μg/mL for itraconazole and voriconazole, 2μg/mL for posaconazole; >16μg/mL for caspofungin, and 0.03μg/mL for terbinafine. No accumulation of liquid or gas was observed on ultrasound. The ulcer started to heal after treatment with amphotericin B 100mg daily for 10 days combined with surgical debridement of the wound. Re-epithelization occurred 3 months after topical application of silver sulfadiazine (Fig. 2).


Fungi of the order Mucorales are ubiquitous in nature, and can be found in soil, organic substrates (wood, fruit, excrements, etc.) or as pathogens in animals and plants.1 Approximately 70% to 80% of Mucorales infections in humans are caused by Rhizopus, Mucor, or Lichtheimia genera and tend to affect immunodepressed individuals. Infections progress fast, do not respond to standard antifungals, and have high morbidity and mortality. The remaining 20% to 30% of cases are caused by the rarer genera Cunninghamella, Rhizomucor, Saksenaea, Apophysomyces, Syncephalastrum, Cokeromyces, and Actinomucor. Infections in these cases tend to run a benign course, with exclusive skin and subcutaneous tissue involvement. They are associated with low mortality and respond well to amphotericin B and azoles.2
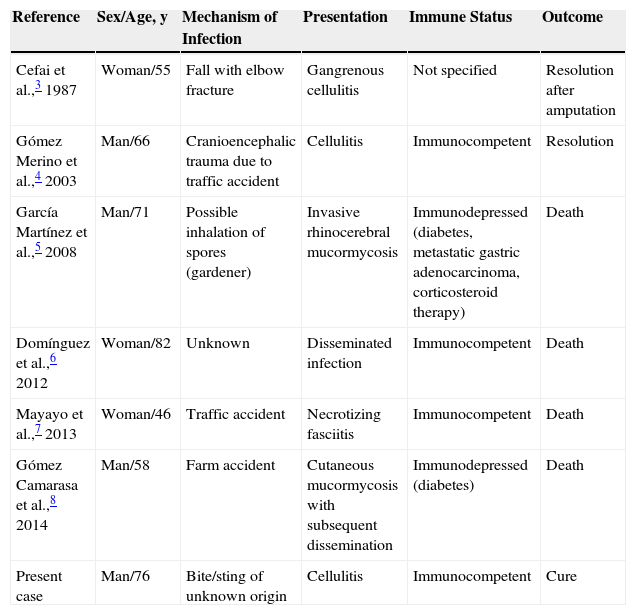
Infections due to S vasiformis have been reported worldwide, although most cases have been described in the United States, Central America, Brazil, Europe, India, and Australia.2 In our search of PubMed, we found 6 cases of S vasiformis infection reported for Spain.3–8 One of these was in the same area as our hospital,6 and they all occurred in adults aged over 45 years (Table 1). In most of the cases, the fungus had penetrated the skin following an accident involving contact with soil. The cases involving local cutaneous involvement were resolved by administration of specific treatment or amputation of the affected limb.3,4 The patients with noncutaneous forms of S vasiformis infection forms died regardless of their underlying immune status.
Published Cases of Saksenaea vasiformis Infection in Spain.
| Reference | Sex/Age, y | Mechanism of Infection | Presentation | Immune Status | Outcome |
|---|---|---|---|---|---|
| Cefai et al.,3 1987 | Woman/55 | Fall with elbow fracture | Gangrenous cellulitis | Not specified | Resolution after amputation |
| Gómez Merino et al.,4 2003 | Man/66 | Cranioencephalic trauma due to traffic accident | Cellulitis | Immunocompetent | Resolution |
| García Martínez et al.,5 2008 | Man/71 | Possible inhalation of spores (gardener) | Invasive rhinocerebral mucormycosis | Immunodepressed (diabetes, metastatic gastric adenocarcinoma, corticosteroid therapy) | Death |
| Domínguez et al.,6 2012 | Woman/82 | Unknown | Disseminated infection | Immunocompetent | Death |
| Mayayo et al.,7 2013 | Woman/46 | Traffic accident | Necrotizing fasciitis | Immunocompetent | Death |
| Gómez Camarasa et al.,8 2014 | Man/58 | Farm accident | Cutaneous mucormycosis with subsequent dissemination | Immunodepressed (diabetes) | Death |
| Present case | Man/76 | Bite/sting of unknown origin | Cellulitis | Immunocompetent | Cure |
These opportunistic fungi gain entry through injuries or wounds caused by trauma, with most cases involving major trauma, such as traffic accidents, farming accidents (wound contamination) and surgery. There have, however, also been descriptions of infections by Mucorales fungi following minor trauma, including bites and stings. There have been reports of S vasiformis infection in a patient pecked by a magpie9 and stung by a scorpion.10 The first case was resolved by wound debridement and administration of amphotericin B, although a skin graft was required to repair the wound defect. In the second case, amputation of the affected leg was necessary.
Infections due to S vasiforms are probably underdiagnosed as these fungi do not easily produce spores in standard fungal media. A high index of clinical suspicion is therefore necessary to ensure early treatment and avoid amputations and fatal outcomes.
Please cite this article as: Coronel-Pérez I, Rodríguez-Rey E, Castilla-Guerra L, Domínguez M. Mucormicosis cutánea primaria por Saksenaea vasiformis en paciente inmunocompetente. Actas Dermosifiliogr. 2015;106:516–518.



