

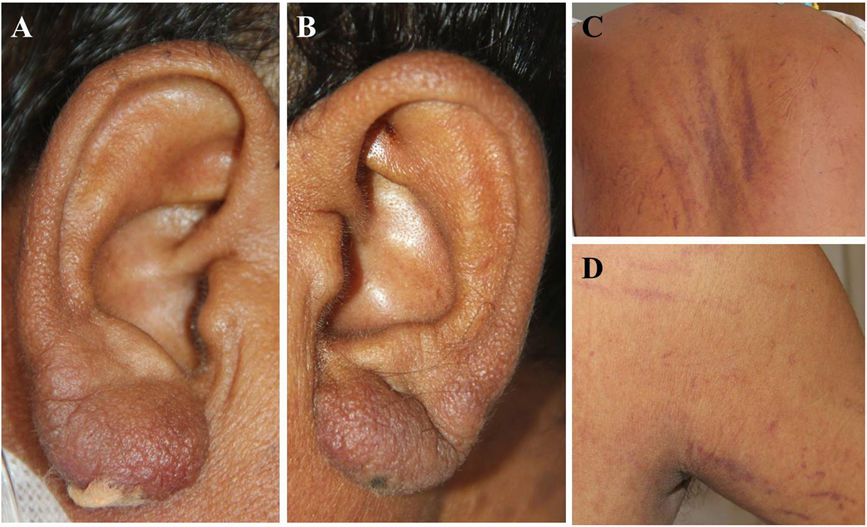
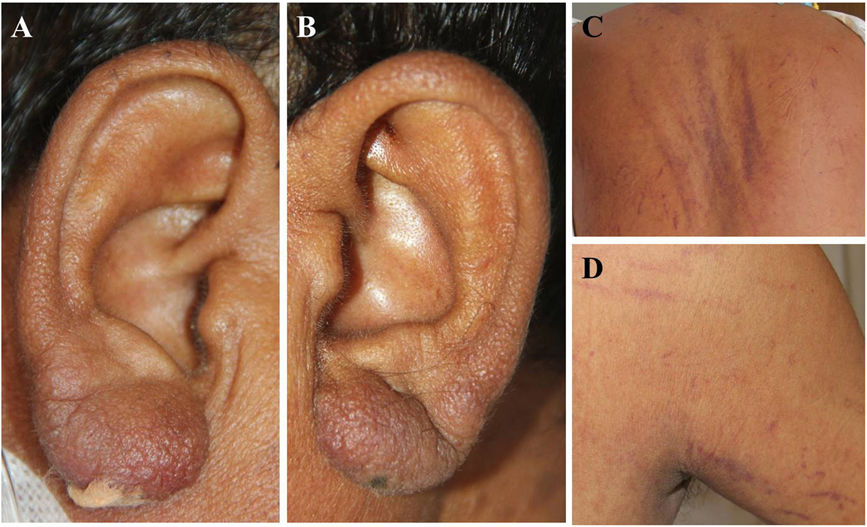
A 45-year-old male presented with intermittent fever, loss of weight and appetite for 2 months. On examination he had generalised lymphadenopathy, faint erythematous infiltration of the earlobes (Fig. 1A and B), and non-palpable, linear purpuras (vibices) involving the trunk and extremities (Fig. 1C and D).
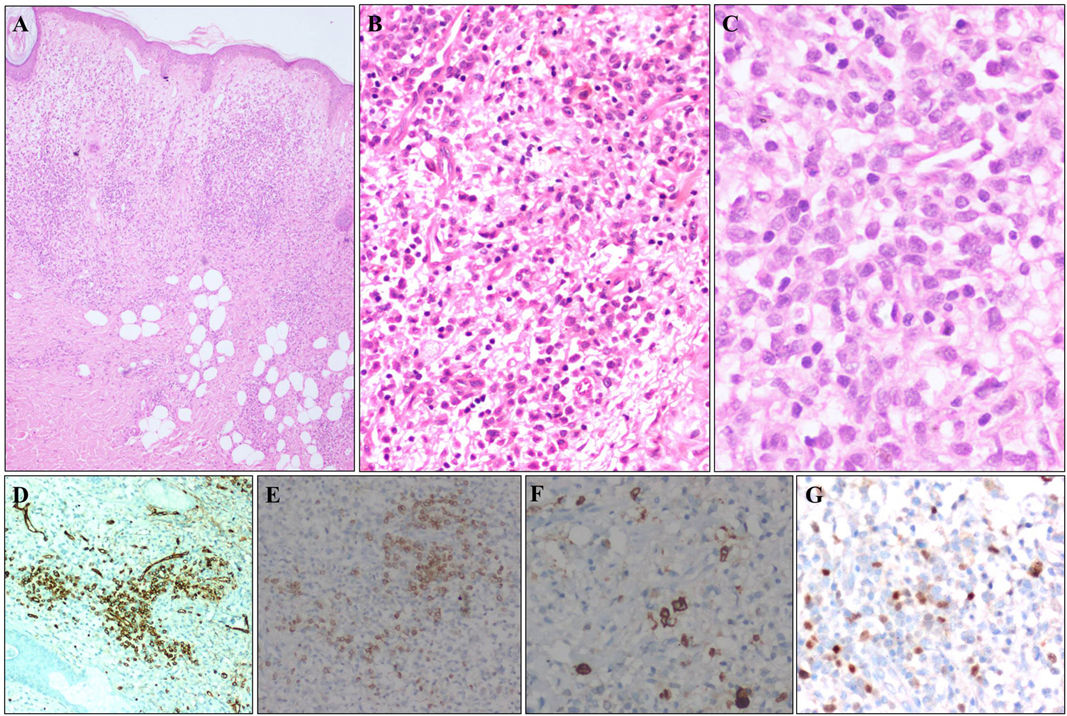
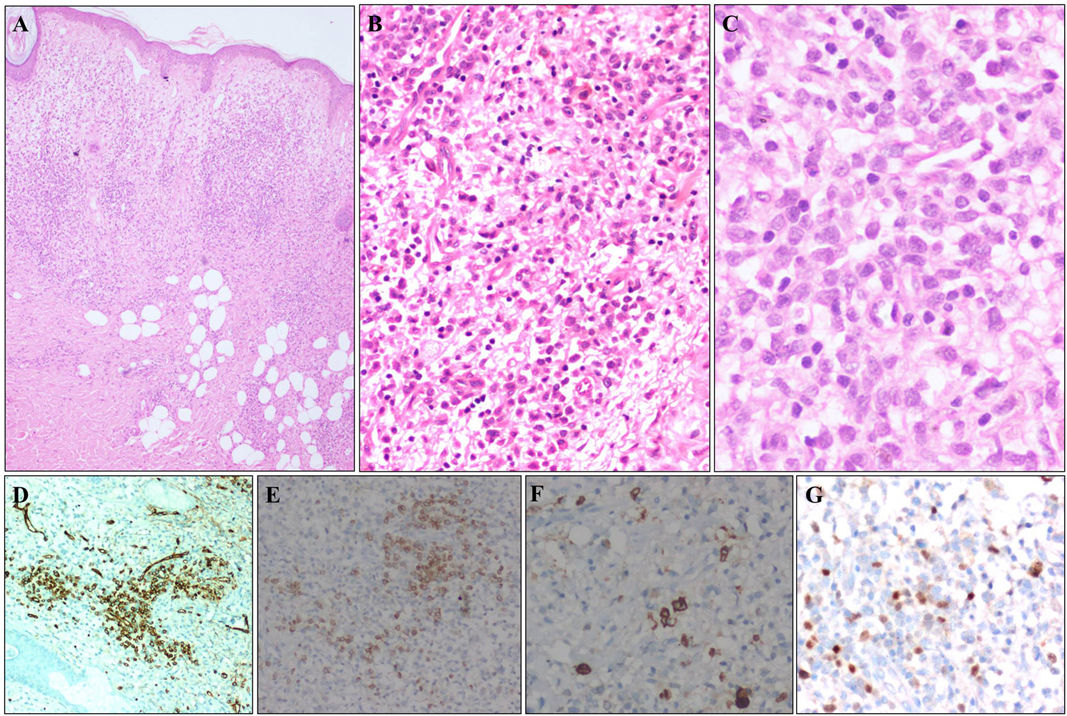
Slit skin smears were negative for acid-fast bacilli. Biopsy from right earlobe revealed moderate-dense dermal infiltrate of atypical lymphocytes displaying high nuclear-to-cytoplasmic ratio (Fig. 2A–C), positive for CD34 (Fig. 2D), CD7 (Fig. 2E), myeloperoxidase (Fig. 2F), TdT (Fig. 2G), consistent with leukemia cutis (LC). Blast cells were detected in peripheral smear (18%) and bone marrow aspirate (85%) and immunophenotyping was consistent with early T-cell precursor acute lymphoblastic leukemia (ALL). Extramedullary involvement was absent and he was initiated on adult ALL protocol.
The cutaneous infiltration of leukemic cells in systemic leukemia or LC may manifest as solitary/multiple, localised/disseminated papules, nodules, and plaques, with rare reports of other morphological presentations, often mimicking non-specific skin lesions of leukemia. It is more common among elderly, males, with acute myeloid leukemia or chronic lymphocytic leukemia (CLL).1
Earlobe infiltration is an intriguing, localised presentation of LC, previously reported in CLL, but not in ALL.2 Biopsy was crucial in excluding other clinical differentials like leprosy, lymphomas, pseudolymphomas, granulomatous rosacea, lupus vulgaris, sarcoidosis, chilblain lupus.



