


Fungiform papillae of the tongue are small projections involved in taste function that are typically located on the lateral aspects and tip of the tongue. They are called fungiform papillae because of their close resemblance to a fungus. In fair-skinned individuals, they are usually pink or red, but in dark-skinned individuals, they are frequently pigmented and are considered a variant of normal oral pigmentation.1 We report a case of pigmented fungiform papillae of the tongue (PFPT) and describe its dermoscopic features, which have been rarely reported in the literature.
A 30-year-old black woman with no personal or family history of interest was evaluated for a pigmented lesion with no apparent cause on the tongue. The lesion had appeared in adolescence but had remained stable and asymptomatic (Fig. 1). The patient was not taking any regular medication, did not smoke, had not had dental treatment in the area of the papillae, and had adequate oral hygiene. The rest of the physical examination was unremarkable.

Dermoscopy showed several projections with hyperpigmented edges whose surfaces contained vessels that emerged from the base forming successive branches resembling rose petals. This rose petal pattern was previously described by Mukamal et al.2 in PFPT (Fig. 2). Another report of the dermoscopic features of PFPT referred to a cobblestone or cobblestone-like pattern,3 but we believe that this is less accurate as the lesion is not a nevus.

PFPL are located on the tip, dorsum, and/or lateral aspects of the tongue, and are distributed among filiform papillae. They are typically red or pink, although a brown variant has been reported. Most cases of PFPT in the literature have been described in Afro-American patients, suggesting that black individuals are more susceptible to this condition than other races.1 The pigmentation is limited to the fungiform papillae, and lesions usually appear in childhood, do not progress, and remain asymptomatic.
The differential diagnosis should include other pigmented lesions of the oral mucosa, such as those seen in hemochromatosis, pernicious anemia, amalgam tattoo, and Addison disease. In all cases, however, a clear diagnosis can be established based on either the clinical features and distribution of the lesions or the accompanying manifestations.4
The pathogenesis of PFPT is unknown, and it is also unclear why only the fungiform papillae are affected; treatment is not necessary due to the benign nature of the condition.4
Histologic examination may or may not reveal pigmentation of basal keratinocytes with abundant melanophages in the lamina propria; this finding corresponds to the pigmented structures seen in dermoscopy.1,3
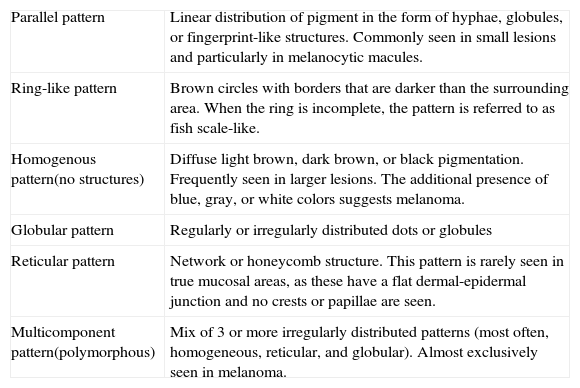
Although dermoscopy is now widely used in clinical practice, few studies have described the dermoscopic features of pigmented oral lesions, and most reports have focused on vulvar lesions. Several characteristic dermoscopic patterns have been described for oral mucosal lesions, and they can all occur in either benign or malignant lesions. Benign lesions can have one pattern or several patterns (in up to 56% of cases) with a regular distribution, while melanomas tend to have several patterns, which in addition are irregularly distributed. The main patterns described to date are summarized in Table 1.5,6
Dermoscopic Patterns of Melanocytic Lesions of the Mucosa.
| Parallel pattern | Linear distribution of pigment in the form of hyphae, globules, or fingerprint-like structures. Commonly seen in small lesions and particularly in melanocytic macules. |
| Ring-like pattern | Brown circles with borders that are darker than the surrounding area. When the ring is incomplete, the pattern is referred to as fish scale-like. |
| Homogenous pattern(no structures) | Diffuse light brown, dark brown, or black pigmentation. Frequently seen in larger lesions. The additional presence of blue, gray, or white colors suggests melanoma. |
| Globular pattern | Regularly or irregularly distributed dots or globules |
| Reticular pattern | Network or honeycomb structure. This pattern is rarely seen in true mucosal areas, as these have a flat dermal-epidermal junction and no crests or papillae are seen. |
| Multicomponent pattern(polymorphous) | Mix of 3 or more irregularly distributed patterns (most often, homogeneous, reticular, and globular). Almost exclusively seen in melanoma. |
The most common patterns in benign pigmented mucosal lesions are globular (25%), homogeneous (25%), fish scale-like (18.8%), and hyphal (18.8%), while in mucosal melanoma lesions they are the multicomponent pattern (75%) and the homogeneous pattern (25%).7
Just one other study to date has described the rose petal pattern observed in our patient as a typical dermoscopic feature of PFPL, and the authors suggested that its presence, in the absence of other alterations, might rule out malignancy.2
We found a close resemblance between the rose petal structure seen in PFPT and the ring-like pattern seen in pigmented melanocytic mucosal lesions. We thus propose that the rose petal pattern should be considered a subtype of the ring-like pattern, as there is also histologic overlapping, with both entities containing pigment deposits in the stroma.
Please cite this article as: Pinos-León V. Características dermatoscópicas de las papilas fungiformes pigmentadas de la lengua. Actas Dermosifiliogr. 2015;106:593–594.



