


Darier disease is a rare autosomal dominant genetic disorder that presents with reddish-brown keratotic papules in seborrheic areas as well as with palmoplantar, nail, and mucosal tissue involvement.1 Darier disease is due to a mutation in the sarcoplasmic/endoplasmic reticulum calcium ATPase gene (ATP2A2), which codes for the endoplasmic reticulum ATPase calcium pump (SERCA2b).1,2 Few case series of patients with Darier disease have been published to date.2 We describe a series of Spanish patients with this disease in the interest of learning more about its characteristics.
To that end we searched our hospital’s database to identify patients diagnosed with histologically confirmed Darier disease treated in our department between January 2008 and January 2019. We extracted the following information for the 20 cases found: age, sex, family history of Darier disease, location of lesions, and concurrent conditions (whether cutaneous or extracutaneous) (Table 1).
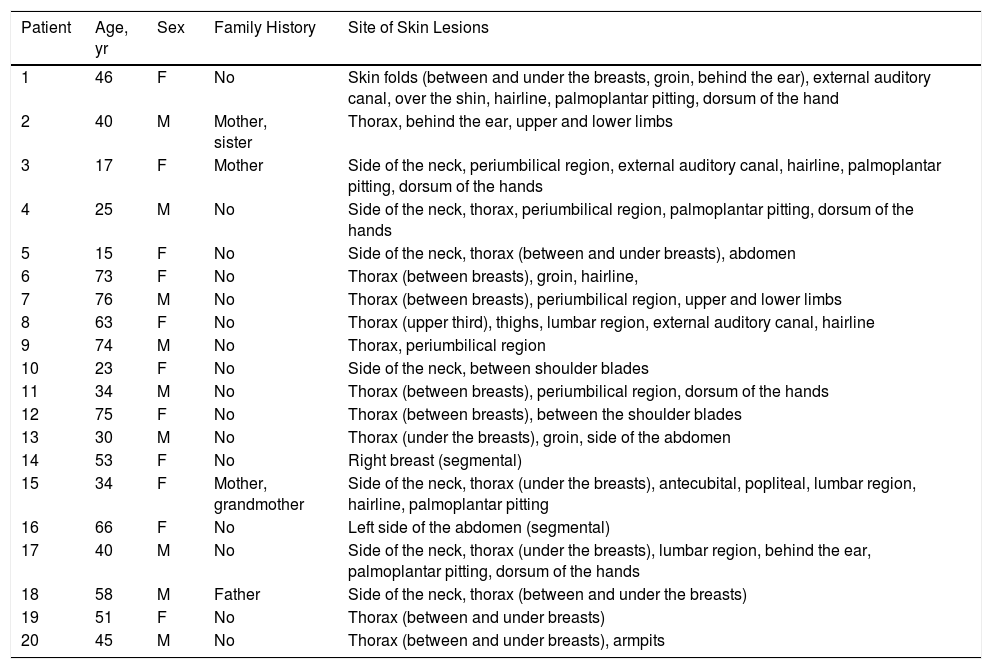
Patient and Lesion Characteristics
| Patient | Age, yr | Sex | Family History | Site of Skin Lesions |
|---|---|---|---|---|
| 1 | 46 | F | No | Skin folds (between and under the breasts, groin, behind the ear), external auditory canal, over the shin, hairline, palmoplantar pitting, dorsum of the hand |
| 2 | 40 | M | Mother, sister | Thorax, behind the ear, upper and lower limbs |
| 3 | 17 | F | Mother | Side of the neck, periumbilical region, external auditory canal, hairline, palmoplantar pitting, dorsum of the hands |
| 4 | 25 | M | No | Side of the neck, thorax, periumbilical region, palmoplantar pitting, dorsum of the hands |
| 5 | 15 | F | No | Side of the neck, thorax (between and under breasts), abdomen |
| 6 | 73 | F | No | Thorax (between breasts), groin, hairline, |
| 7 | 76 | M | No | Thorax (between breasts), periumbilical region, upper and lower limbs |
| 8 | 63 | F | No | Thorax (upper third), thighs, lumbar region, external auditory canal, hairline |
| 9 | 74 | M | No | Thorax, periumbilical region |
| 10 | 23 | F | No | Side of the neck, between shoulder blades |
| 11 | 34 | M | No | Thorax (between breasts), periumbilical region, dorsum of the hands |
| 12 | 75 | F | No | Thorax (between breasts), between the shoulder blades |
| 13 | 30 | M | No | Thorax (under the breasts), groin, side of the abdomen |
| 14 | 53 | F | No | Right breast (segmental) |
| 15 | 34 | F | Mother, grandmother | Side of the neck, thorax (under the breasts), antecubital, popliteal, lumbar region, hairline, palmoplantar pitting |
| 16 | 66 | F | No | Left side of the abdomen (segmental) |
| 17 | 40 | M | No | Side of the neck, thorax (under the breasts), lumbar region, behind the ear, palmoplantar pitting, dorsum of the hands |
| 18 | 58 | M | Father | Side of the neck, thorax (between and under the breasts) |
| 19 | 51 | F | No | Thorax (between and under breasts) |
| 20 | 45 | M | No | Thorax (between and under breasts), armpits |
The patients’ median age of 46 (range, 15–76) years was slightly higher than the ages reflected in the literature, where symptoms debut in patients between 12 and 20 years old; the distribution of sexes in our series was similar, however.3 A family history of Darier disease was reported by 20% of our patients, a lower proportion than the 50% to 60% reported in the literature.1
The most common clinical manifestation was the presence of brownish, keratotic, or erythematous papules that might or might not be grouped in verrucous plaques. We observed the histologic features that are typical of the disease: acantholysis, dyskeratosis, and negative direct immunofluorescence.1–3
Some of the subtypes of Darier disease were represented in our study (Fig. 1). Patient 15 developed reddish-blackish macules on hands and feet, a presentation consistent with the acral hemorrhagic type. Such lesions are caused by bleeding within acantholytic vesicles and may be associated with the p.N767S mutation in the ATP2A2 gene.4 The vesiculobullous variety was seen in patient 17, who had vesicles and blisters mixed with keratotic papules as the primary lesions. In such cases it is important to rule out infection, especially by a virus.5 Patient 11 had comedones and cysts along with keratotic papules, consistent with comedonal Darier disease. This subtype is difficult to diagnose because of its resemblance to acne vulgaris and familial dyskeratotic comedones.6 Two patients had lesions following along the lines of Blaschko (right breast and flank). After biopsy, these cases were confirmed as type 1 segmental Darier disease. This type debuts later in life and must be distinguished from Grover disease and warty dyskeratoma, which are clinically and histologically similar but whose lesions do not present in a blaschkoid distribution.7

Some of the subtypes of Darier disease. A, Acral hemorrhagic Darier disease: dark red macules on the dorsum of the hand. B, Vesiculobullous type: vesicles and blisters of various sizes are present along with erythematous-keratotic papules. C, Comedonal form: comedones and cysts appear along with the typical lesions of Darier disease. D, Type 1 segmental Darier disease: involvement limited to the lines of Blaschko on the left flank.
Although hypopigmented macules intermingled with keratotic papules, a finding referred to as guttate leukoderma, are sometimes present, we saw no such eruptions in our series. Other variants not represented were hypotrophic, verrucous, and erosive forms of Darier disease.
However, multiple associated disorders were present in our series (Table 2). Given that the calcium pump (SERCA2b) is present in all cells, that a genetic mutation would cause symptoms in organs other than the skin seems logical.
Most Common Concomitant Conditions in Our Case Series
| Disease Type | Examples | No. (%) of Patients |
|---|---|---|
| Neuropsychiatric disorders | Epilepsy, hyperactive attention deficit disorder, anxiety-depressive disorder | 6/20 (30%) |
| Dermatologic diseases | Melanoma | 3/20 (25%) |
| Salivary gland disorders | Submandibular sialolithiasis | 1/20 (5%) |
| Kidney diseases | Renal polycystic disease | 1/20 (5%) |
Extracutaneous manifestations of Darier disease, apparently due to the pleiotropic influence of ATP2A2 mutations on other cells, have been described.8 Associated neuropsychiatric disorders were present in 30% of the patients in our series in the form of epilepsy, attention deficit hyperactivity disorder, and anxiety-depressive disorder. Another reported association is salivary gland obstruction caused by episodes of acantholysis and dyskeratosis in the epithelium of salivary ducts.9 Another of our patients had “submaxillary” (ie, submandibular) sialolithiasis that required submaxillectomy. One of our patients had renal polycystic disease, which is also a reported association10; we underline the importance of bearing kidney disease in mind so that it can be diagnosed early.
Finally, 3 patients in our series had melanomas. This association has been described occasionally in the literature but is likely to be a chance finding.1
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Sánchez Martínez EM, Moneva Léniz LM, Gegúndez Hernández H, Mateu Puchades A. Enfermedad de Darier: serie de 20 casos y revisión de la literatura. Actas Dermosifiliogr. 2021;112:675–677.


