


Chronic lip fissure is defined as the presence of a persistent linear ulcer in the sagittal plane of the upper or lower lip. Its prevalence in the general population is 0.57%, and it more frequently affects men than women (4:1).1
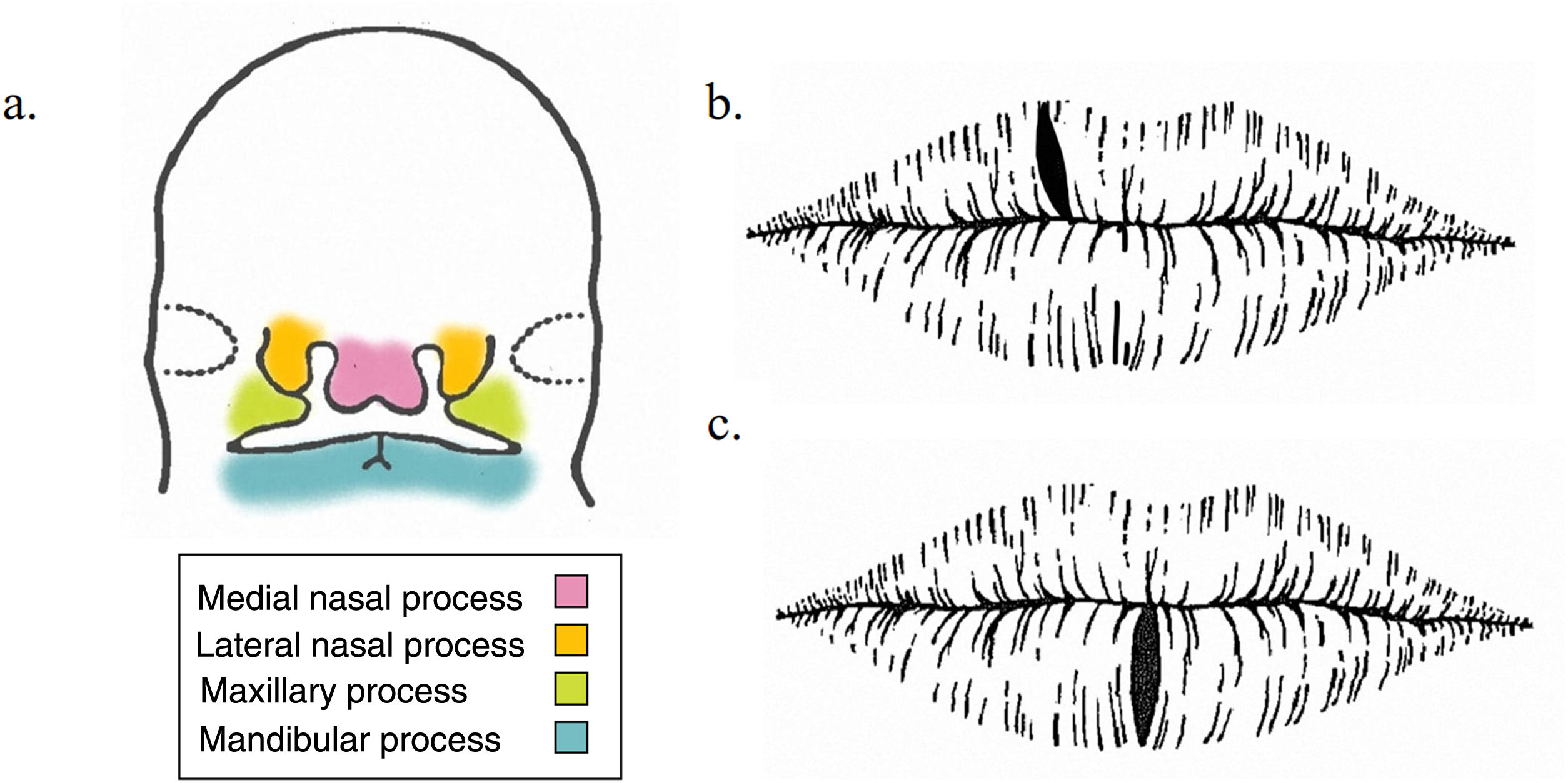
The condition has traditionally been associated with the presence of a physiological weakness at the level of embryonic fusion planes of the first branchial arch, specifically, of the mandibular and/or maxillary processes (Fig. 1A). Therefore, it seems that fissures of the lower lip are found on the midline, whereas those affecting the upper lip are in a more lateral position (Fig. 1B and C).1,2
, whereas those on the lower lip are usually seen on the midline (C).")
Other factors that can predispose to chronic lip fissure include exposure to low temperatures, smoking, breathing through the mouth, malocclusion, local infection, vitamin deficiency, playing wind instruments, Down syndrome, Crohn disease, and facial granulomatosis. Localization and the constant presence of moisture delay spontaneous healing and contribute to the chronic course of the lesion. Chronic lip fissure progresses with pain, bleeding, and cosmetic alterations that may be present continuously or intermittently.3 Similarly, since more than 6% of chronic lip fissures are associated with a risk of malignant transformation, adequate and early management is essential.1
Importance of Z-plasty in the Treatment of Chronic Lip FissureFirst-line treatment of chronic lip fissure is conservative, with corticosteroids, immunomodulators, and antibiotics. However, refractoriness to topical treatment is common, with the result that in cases of failure or recurrence, treatment is with carbon dioxide laser, cryotherapy, or surgery.1 In the case of surgery, the surgeon must avoid simple excision of the fissure with subsequent direct closure: this intervention favors recurrence of the lesion, since the same tension that caused the fissure is maintained. The scar resulting from the procedure creates a notch in the sagittal plane of the lip where the lesion can reappear.2 The problem can be solved by performing Z-plasty instead of simple excision.
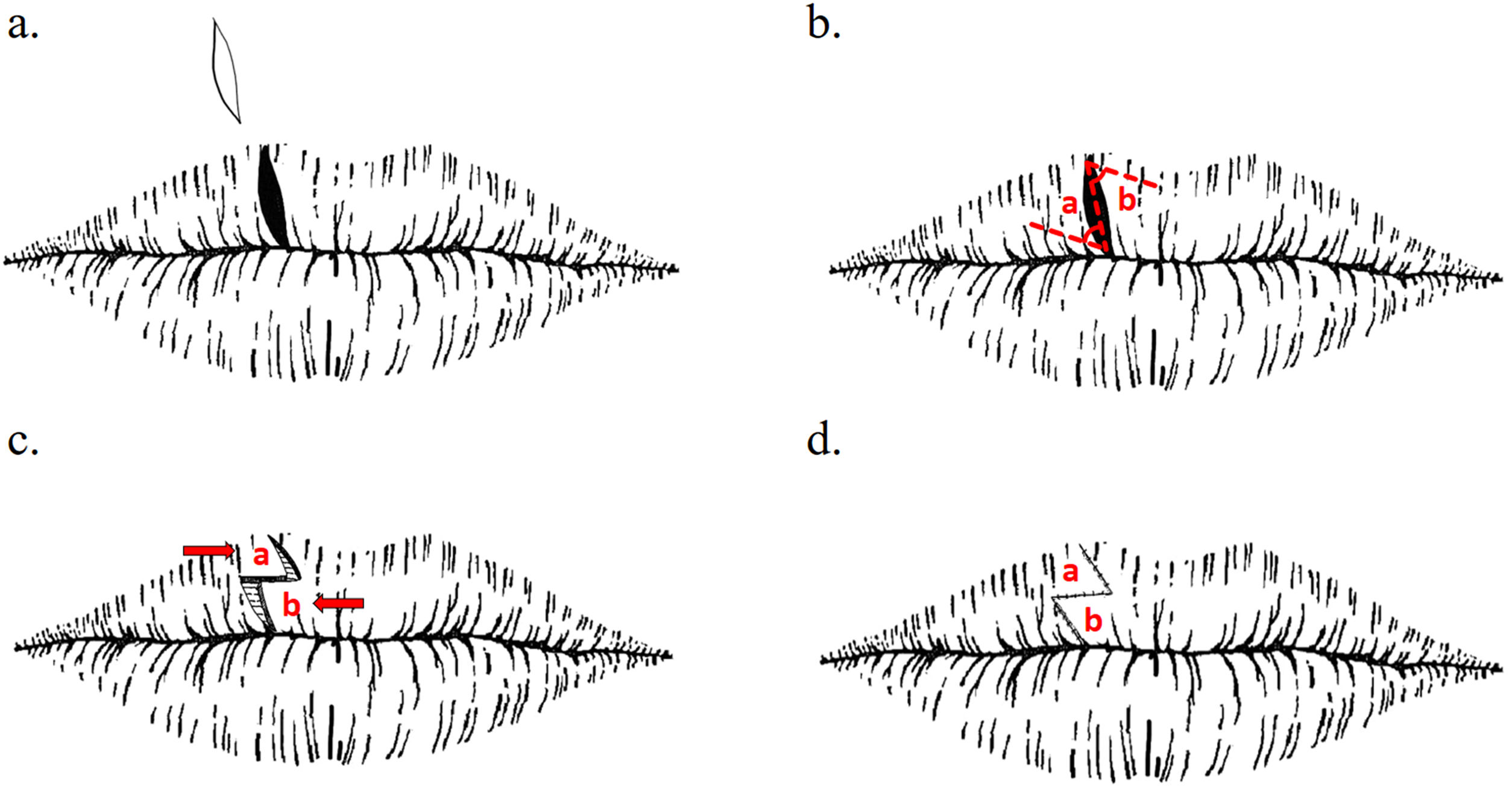
Z-plasty is a double transposition flap. Its design involves 3 segments that are equal in length, with a central segment from which the other 2 segments run in opposite directions and with a variable angle, upon which the eventual length of the scar depends. In our experience, Z-plasty at an angle of 60° yields better cosmetic and functional outcomes, since, even though this angle extends the scar by up to 75%, it provides adequate length to the anatomical area without compromising the irrigation of the flap. Consequently, Z-plasty lengthens the scar and modifies its direction, thus reducing its contraction.4 The technique involves elliptical excision of the fissure, including the buccal mucosa and following the tension lines of the lip (Fig. 2A). The two triangular flaps are then marked and traced with a scalpel (Fig. 2B). Once traced and with the tissue released appropriately, the triangular flaps are transposed contralaterally, and the defect is sutured (Fig. 2C). It is important to spare the limit of the mucocutaneous line when designing the upper flap to avoid transposing hair onto the labial mucosa. Compared with simple excision, Z-plasty is associated with 20% fewer recurrences at 12 months, since by modifying the direction of the scar, we reduce tension in the sagittal plane of the fissure, thus diminishing the probability of recurrence.2,5 The procedure also provides very acceptable short- and long-term cosmetic outcomes, despite more considerable labial edema immediately after the procedure than with simple excision2 (Fig. 3).
 and subsequent design of two triangular flaps, which are traced with a scalpel (B). Once traced and after appropriate release of the tissue, the triangular flaps are transposed contralaterally, and the defect is sutured (C and D).")
The technique involves elliptical excision of the fissure following the tension lines of the lip (A) and subsequent design of two triangular flaps, which are traced with a scalpel (B). Once traced and after appropriate release of the tissue, the triangular flaps are transposed contralaterally, and the defect is sutured (C and D).
. Appearance of the wound immediately after surgery (B), on removal of the stitches, at 1 week (C), and at 2 weeks (D).")
Chronic lip fissure is a relatively common condition that affects the patient's quality of life and carries a significant risk of malignant transformation. Therefore, treatment with surgery is essential. Z-plasty constitutes a more functional and cosmetically pleasing alternative than simple excision.
FundingThe authors declare that no funding was received for the present study.
Conflicts of InterestThe authors declare that they have no conflicts of interest.



