

The scalp ringworm (tinea capitis [TC]) is a highly contagious disease caused by dermatophytes of the Microsporum and Trichophyton genera.1,2 TC often affects children and, although relatively rare, is not exceptionally rare among adults.1,3 In Spain, the most common etiological agents for years have been zoophilic fungi such as Microsporum canis. In the past decade (more clearly identifiable since January 2021 when mycological cultures could be obtained in the clinic referred to in this paper for the first time), there has been a higher incidence of TC due to an anthropophilic species—Trichophyton tonsurans—which, until recently, was rare in our country and the rest of Europe.4
A total of 29 cases of ringworm were diagnosed in the clinic from January 2021 through October 2023, all of which were characterized by the growth of Trichophyton tonsurans. Researching on the possible origin of Trichophyton tonsurans and after seeing similar cases in Germany,5 all patients had a common denominator: they were mostly young men (or contacts of these) who had had a haircut with a graded fade in the occipital and/or temporal region using an electric shaver on a weekly basis. These preferences seemed have been triggered by the hairstyles of celebrities such as professional footballers and actors.6
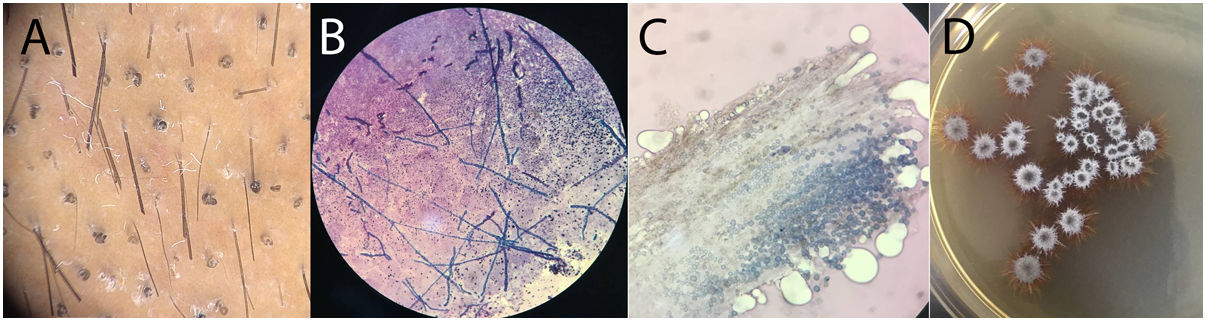
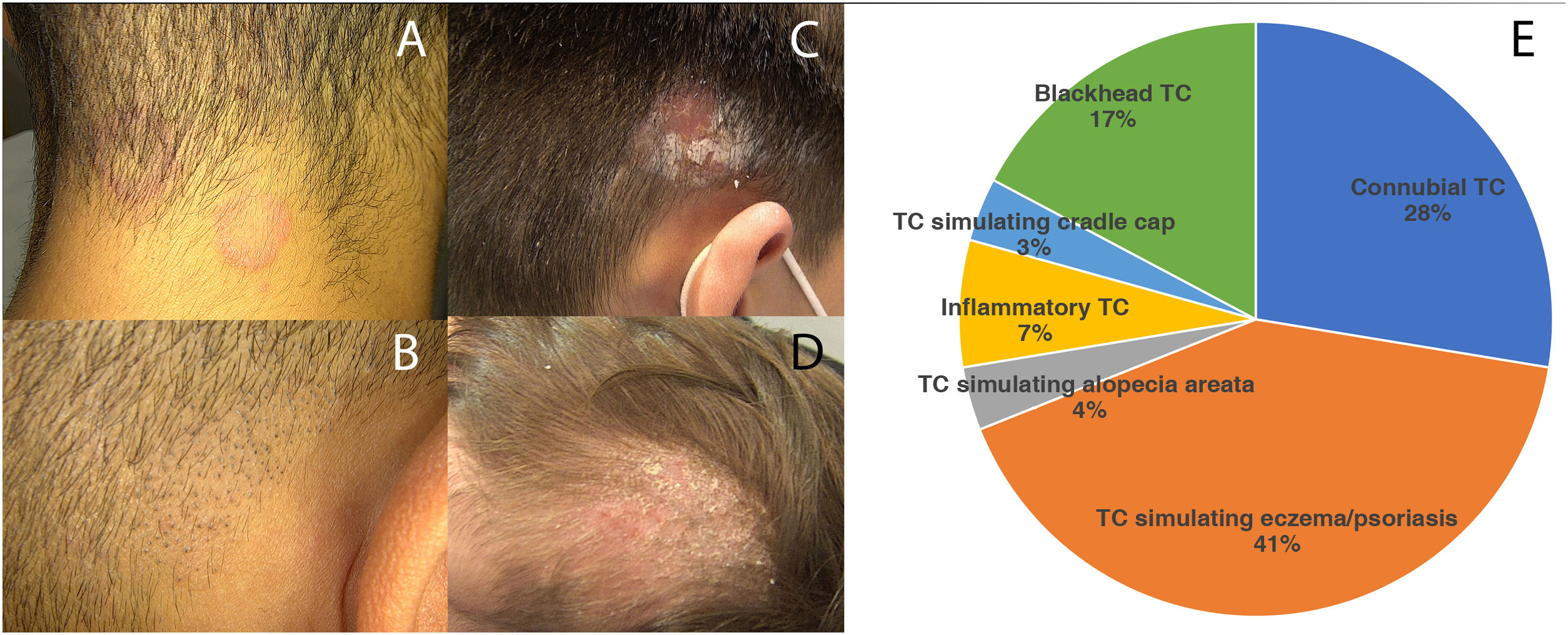
Trichoscopic imaging were obtained from all the patients from the series (Fig. 1A), as well as direct KOH examinations and mycological cultures (Fig. 1B-D). The clinical signs reported included erythematous-scaly lesions in the occipital and/or temporal regions clinically very similar to psoriasis or seborrheic dermatitis, which is why they had previously been treated in other centers with topical corticosteroids in some cases, resulting in worsened lesions (Fig. 2A; also see one of the most striking cases of the series included in panel B-Figure 2 of the references number 6).6 Connubial TC in infected patients from hair salons was also a common finding. Less frequently, patients with black dot TC (Fig. 2B) and inflammatory TC (Fig. 2C) were seen. It was not uncommon that many of these patients (especially those with black dot TC) were asymptomatic carriers, being trichoscopy of great help in their detection.7 Similarly, isolated cases of patients simulating alopecia areata and cradle cap in the youngest female patient of the series were also found (Fig. 2D), whose father, with TC diagnosed in the clinic and acquired at a hair salon, had infected her. All cases were reported to the Provincial Health Delegation of Malaga, Spain (presentation summarized in Fig. 2E) to locate the centers where the infections had occurred to stop the infections from spreading somewhere else.
 Trichoscopic image of corkscrew hairs typical of black dot ringworm. B) Septate hyphae on KOH examination. C) Endothrix parasitization of the hair shaft by the fungus. D) Isolation of T. tonsurans on Sabouraud glucose agar with chloramphenicol.")
 Non-inflammatory forms mimicking seborrheic dermatitis. B) Black dot ringworm. C) Inflammatory form with retroauricular lymphadenopathy. D) Ringworm simulating cradle cap. E) Description of the cases diagnosed in the clinic.")
After the detection of the initial cases in the clinic, the outbreak was reported to the Spanish Dermachat dermatology chat to detect new infections in other parts of Spain and prevent the appearance of new cases.6
The reason for this increased incidence of Trichophyton tonsurans is unknown. However, we believe it has to do with greater immigration flows coming from African countries, where it is particularly common.4 Additionally, some authors have attributed, at least partly, the greater virulence of this pathogen to the use of griseofulvin since the mid-20th century, the only approved oral antifungal treatment in childhood for all forms of scalp ringworm.4,8
Regarding hair salons, there are different regulations in place (sometimes articulated in the form of municipal ordinances) requiring the use of disposable material and, for the lack of that, proper disinfection after use. In this regard, studies published in other countries dealt with the most suitable agents for disinfecting fomites infected with Trichophyton tonsurans.9 Fortunately, this is something that most workers from this sector already do, while trying to make sure that this is done correctly in all hair salons.10
In conclusion, we believe that the communication of this experience may be relevant because it highlights several things: first, that it is possible to conduct a research and contribute to public health from all settings, including small dermatology clinics; second, that dermatologists play an undeniable role in mycology and that large resources are not essential to perform honest and useful investigations. Finally, that we are at a time when the incidence of infections is changing on so many different levels.
We wish to thank Dr. Vicente Crespo Erchiga for being the master of mycology that he is and for his teachings in the art of conducting mycological cultures.



