





Reconstruction of the pharynx after cancer surgery involves different types of skin flaps that contain hair follicles. As the hair in these follicles grows, the patient experiences problems such as swallowing or speech disorders. While the hair is usually removed from the flap before surgery, this is not always the case.1 Laser hair removal is commonly applied to skin, although it is not designed for use in cavities. Cases involving the mouth2 and layrnx3 have been reported. We present an unusual case of laser hair removal from a hairy flap in the hypopharynx after reconstructive surgery for squamous cell carcinoma.
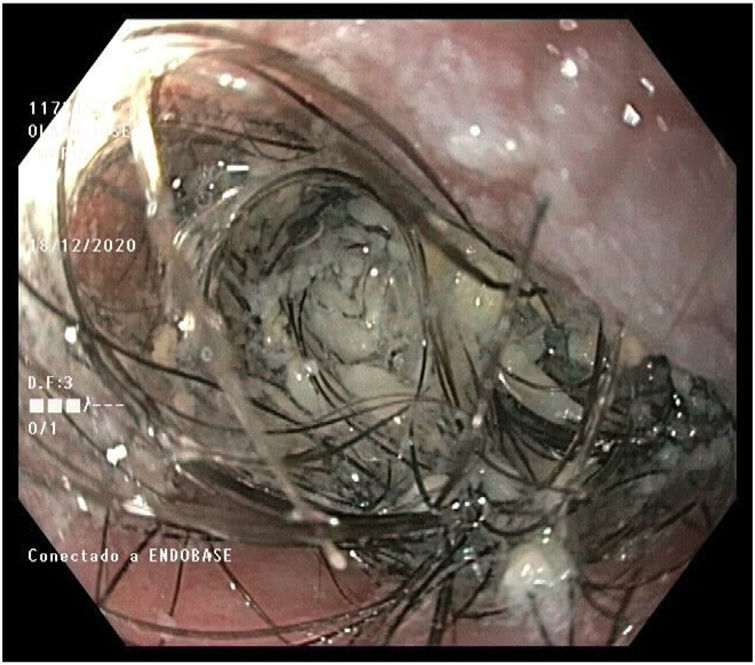
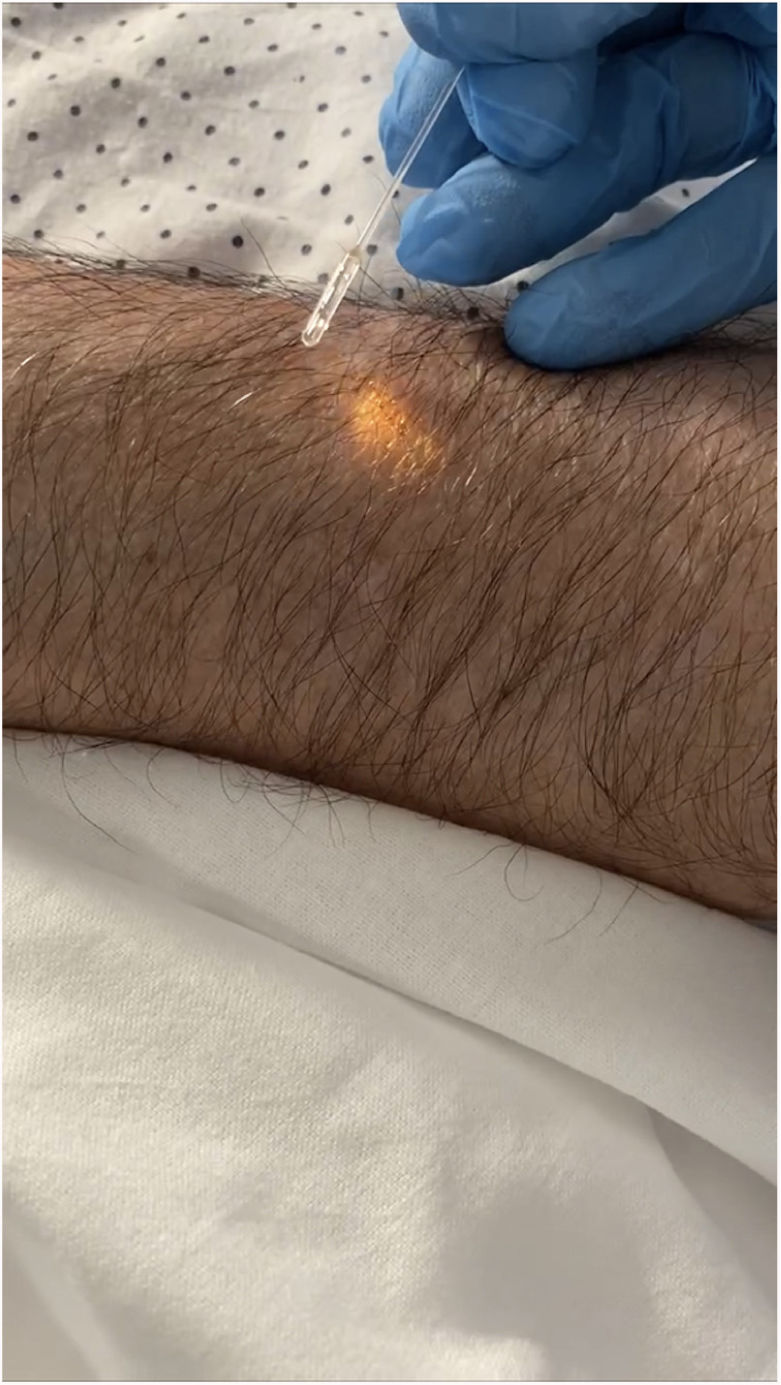
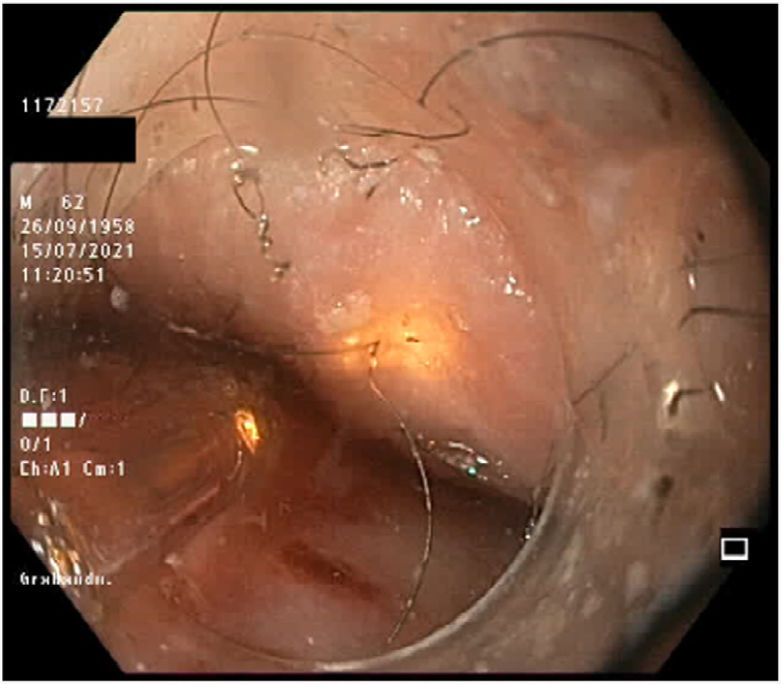
The patient was a 62-year-old man who was diagnosed with squamous cell carcinoma of the hypopharynx (T3N2c, stage IVA) in 2018. He underwent radical laryngectomy and node removal in 2019, followed by radiochemotherapy. The resulting defect was resolved in 2 stages with a myocutaneous flap from the right pectoralis major in October 2019 and left pectoralis major in January 2020. The graft was 270° in circumference and 3cm long, creating a neopharynx anastomosed to the cervical esophagus. Some months after the procedure, the patient complained of dysphagia. Gastroscopy revealed a large tangle of hairs on the graft that prevented passage of the endoscope (Fig. 1). Treatment was with a 755-nm alexandrite laser (Duetto MT Evo, Quanta System) using a 600-μ laser fiber measuring 3 m in length to pass through the endoscope, with lateral light emission to deliver shots in a tubular space (Fig. 2). Tests were performed on the patient's skin to set pulse durations and fluences that did not burn and proved effective. Treatment was administered under general anesthesia. Oxygen was maintained at 21% during the procedure to prevent combustion. The laser fiber was inserted into a gastroscope measuring 1030mm in length and 9.9mm in diameter with a working channel measuring 2.8mm in diameter. The laser guide light was aimed perpendicular to the point of exit of each hair. The parameters applied were as follows: spot size, 4mm; fluence, 16J/cm2; pulse duration, 15ms. No cooling system was used. A total of 900 shots were delivered. The hair in this area was removed pending further sessions (Fig. 3). The second session was 7 months after the first, and the amount of hair had decreased. During this session, the hair was removed at a higher energy (18J/cm2), and 800 shots were delivered. After the session, it was possible to pass the endoscope to the duodenum through a tortuous area resulting from surgery and not the hair.
Laser hair removal from a hairy flap has been reported after reconstructive surgery. The procedure is nearly always performed in the oral cavity owing to its accessibility. Kuriloff et al.4 used a CO2 laser to remove hair from a hypopharyngeal flap. Since then, hair removal has been performed in the mouth using specific epilating lasers such as the neodymium-yttrium aluminum garnet laser5,6 and the alexandrite laser.2,7 On one occasion, hair was removed from a laryngeal flap using a 980-nm diode laser.3
We opted for the alexandrite laser owing to its effectiveness, our experience, and the properties of the laser, which prevent it from reaching deeper areas and include the almost nonexistent risk of burning. The parameters we applied were based on previous tests performed on animal skin and on tests performed on the patient himself (skin on the chest and forearm, which was finer).
In our procedure, treatment was delivered perpendicular to the wall of the pharynx at the point of exit of each hair follicle, one by one, in order to attain a perfect circle that would distribute the light energy appropriately. Before removal, the longest hairs were cut with endoscopy scissors; the remainder were treated directly with the laser. The broken epilated hairs were removed with endoscopy forceps.
Treatment made it possible to reduce the amount of hair and view potential postsurgical stenosis. Given that the patient is still being fed via gastrostomy, we were unable to evaluate whether swallowing had improved. We administered treatment in 2 sessions. Dysphagia improved after the second session, and the patient was able to ingest water and purées. Follow-up gastroscopy is pending to determine whether a third session is necessary.
Treatment was administered with general anesthesia owing to the estimated duration (900 shots). Unlike Min Woo Park et al.,3 we were unable to administer local anesthetic.
Laser hair removal from a skin flap before reconstruction is a simple technique that helps to avoid the problem described here.1
The approach we describe is pioneering because it involves the placement of a laser to remove hair in the pharynx. It may prove useful in similar cases and should draw attention to the need for epilation of skin flaps before surgery.
FundingThe authors declare that no funding was received for the present study.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
This treatment was designed and performed by 10 professionals from different specialties. We are grateful both to them and to the patient for his availability and patience.


