



To assess the level of agreement on various prevention and management strategies for irritation caused by topical retinoids in facial and trunk acne in an attempt to alleviate it and minimize treatment discontinuations as much as possible.
MethodAfter reviewing the scientific medical literatura currently available, 4 different areas of uncertainty in the management of irritation caused by topical retinoids in acne were identified. A questionnaire with 34 recommendations was created and evaluated by a group of 133 dermatologists (Delphi methodology).
ResultsIn 82.3% of the recommendations (28 out of 34), some level of agreement was reached (≥85% agreement in 22 recommendations and≥70% agreement in 6). The results with the highest level of agreement focused on specific patient education strategies (explaining that irritation is an expected reaction at the beginning of treatment and tends to decrease over time), gradual and/or spaced application of topical retinoids (at night time to prevent and/or reduce skin irritation), and the importance of using adjuvant products, specific for acne-prone skin, hydration, photoprotection, and skin cleansing. These recommendations reflect a comprehensive approach to managing irritation associated with topical retinoids and promoting long-term adherence.
ConclusionsSkin irritation caused by topical retinoids in facial and trunk acne is an expected, mild, and controllable reaction if proper prevention and management guidelines are followed, meaning that it should not be a reason for treatment discontinuation.
Conocer el grado de acuerdo en diversas estrategias de prevención y manejo de la irritación por retinoides tópicos en acné facial y troncal con la finalidad de mejorarla y evitar, en la medida de lo posible, abandonos de tratamientos.
MétodoTras revisar la literatura, se identificaron 4 áreas de incertidumbre en el manejo de la irritación por retinoides tópicos en acné. Se desarrolló un cuestionario con 34 recomendaciones que fueron evaluadas por un grupo de 133 dermatólogos (metodología Delphi).
ResultadosEn un 82,3% de las recomendaciones (28 de 34) alcanzó algún grado de acuerdo (22 consenso con≥85% de acuerdo y 6 mayoría con≥70% de acuerdo). Los resultados con mayor grado de acuerdo se centraron en estrategias específicas de educación del paciente (explicar que la irritación es una reacción esperable al inicio del tratamiento y que tiende a disminuir con el tiempo), aplicación gradual y/o espaciada de los retinoides tópicos (por la noche para prevenir y/o reducir la irritación de la piel) y la importancia de usar productos adyuvantes, específicos para piel con acné, para la hidratación, fotoprotección y limpieza de la piel. Estas recomendaciones reflejan un enfoque integral para gestionar la irritación asociada a retinoides tópicos y fomentar su adherencia a largo plazo.
ConclusionesLa irritación de la piel por retinoides tópicos, en acné facial y troncal, es una reacción esperable, leve y controlable si se siguen unas correctas pautas de prevención y manejo, y no debería ser motivo de abandono del tratamiento.
Acne is a highly prevalent chronic inflammatory disease worldwide, affecting approximately 80% of adolescents (from 13 to 18 years old)1 that usually grows into adulthood. In its most severe or persistent forms, it leads to a series of psychosocial effects that can negatively impact the patient's quality of life.2
Currently, retinoids (both oral and topical) are the gold standard to treat acne as first-line therapy according to the main national and international clinical practice guidelines.3–6
The first topical retinoid for acne therapy was tretinoin, also known as retinoic acid, which was approved by the U.S. Food and Drug Administration (FDA) in the 1970s.7 Since then, other retinoids such as isotretinoin, adapalene, and trifarotene have also been approved and are currently marketed in Spain and Portugal to treat acne.8
Retinoids work by activating nuclear retinoic acid receptors in the skin. These receptors regulate gene expression, which in turn can improve cell turnover, reduce sebum production, and increase collagen production.9 However, this process can also cause skin irritation. Retinoids can increase the production of enzymes that degrade collagen and skin proteins, leading to dryness, peeling, and redness. Additionally, retinoids can alter the skin lipid barrier, making it more susceptible to water loss and, therefore, drier, more sensitive, and more prone to irritation.10,11
Although skin irritation is considered a sign that treatment is working,12 as it indicates that the skin is experiencing faster cell turnover, excessive irritation can be counterproductive and cause the patient to abandon the treatment.13
In our routine dermatological clinical practice, we are used to managing the tolerability issues associated with retinoids, using different strategies to minimize potential irritation. These include: 1) training the patient on the correct application of treatment, especially within the first few weeks, and 2) using cosmetics as adjuncts to maintain proper hygiene and hydration of the affected area.
However, literature supporting these strategies is scarce, as well as information on how to properly prevent or efficiently treat tolerability issues associated with topical retinoids in facial and truncal acne. This knowledge and these skills should become part of the expertise of all health professionals involved in the management of acne.
The objective of this consensus document was to validate a series of recommendations aimed at improving the approach to patients with acne and the tolerability of topical retinoid therapies. We consider these recommendations of great interest to health professionals often dealing with acne patients, including dermatologists, general practitioners, and pediatricians.
MethodSelection of participantsOne scientific committee for the project was established, including 8 dermatologists (7 Spanish and 1 Portuguese) focused on facial and truncal acne. The committee, with methodological assistance, defined the objectives, scope, and sections of the document. Four major topic groups were addressed: 1) preferences for topical acne treatment; 2) skin irritation and topical acne treatment with retinoids; 3) recommendations/guidelines to prevent/reduce skin irritation in topical acne treatment with retinoids; and 4) extreme weather conditions and skin irritation and topical acne treatment with retinoids.
Literature review and preliminary recommendationsA literature review (PUBMED and COCHRANE) on recommendations and strategies to improve the tolerability of topical retinoids in acne treatment was conducted. With the information obtained, the scientific committee created a series of preliminary recommendations.
Scientific committee meetingsThe scientific committee met twice to review and confirm the objectives, scope, and sections of the document. Subsequently, the results of the literature review and the provisional recommendations were presented and discussed. This led to the definition of 34 final recommendations.
DelphiThe 34 final recommendations were subjected to consensus using the Delphi method14 to establish the level of agreement on such recommendations.
This was done online through Google Forms and, in addition to the scientific committee, these recommendations were submitted to 125 dermatologists (108 Spanish and 17 Portuguese). Votes were cast on a Likert scale15 from 1 (totally agree) to 5 (totally disagree). Consensus was defined when, at least, 85% of participants voted ≤ 2 (totally agree and agree), and majority when, at least, 70% of participants voted ≤ 2. Recommendations with a level of agreement <85% in the 1st round of voting were voted in a 2nd Delphi round (the cutoff values did not change from the 1st to the 2nd Delphi round). This methodology was selected due to its common and recent use in the field of acne.16,17
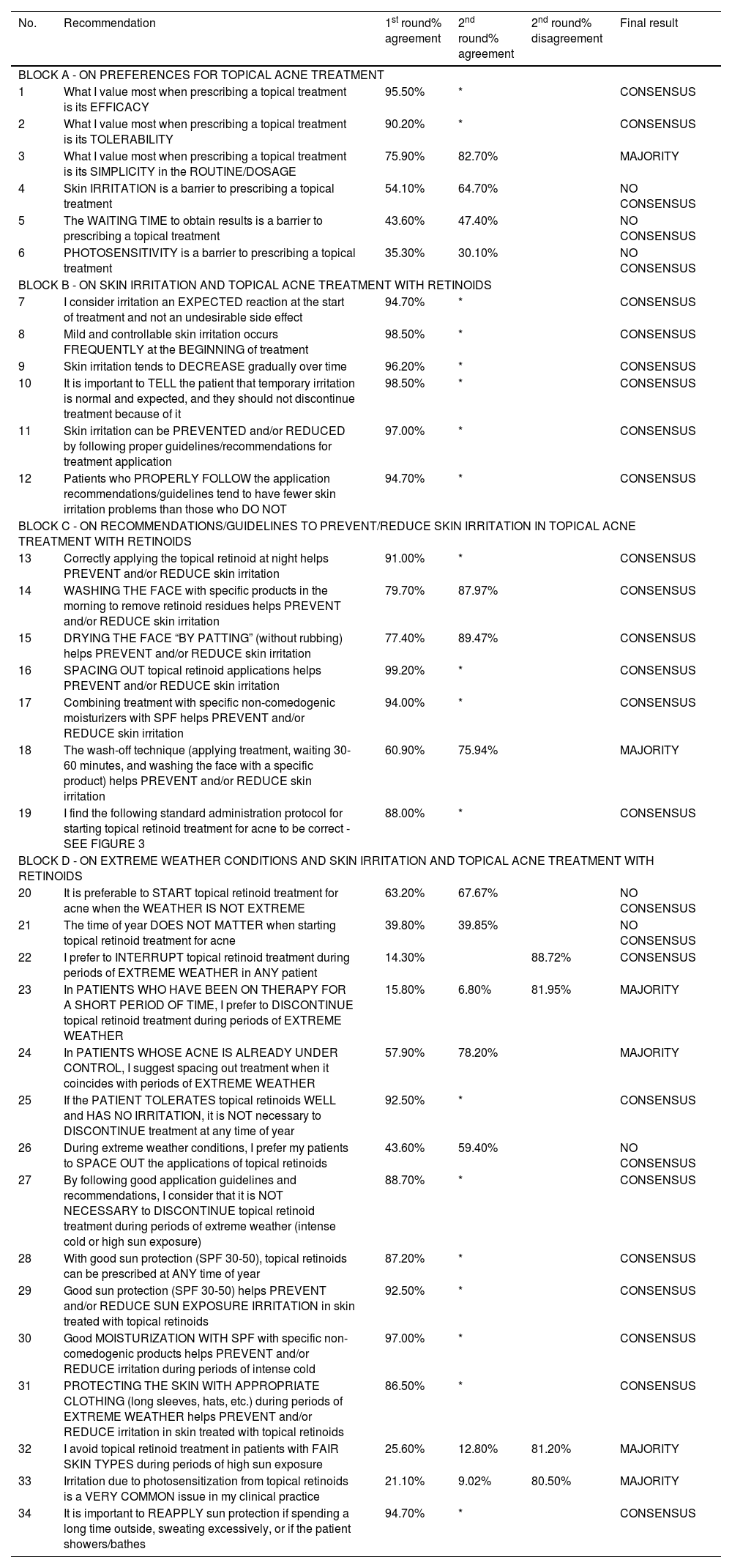
ResultsConsensus was reached on 22 recommendations (64.70%), 19 in the 1st round and 3 in the 2nd round. A total of 6 recommendations (17.65%) achieved a majority consensus, as opposed to another 6 (17.65%) which did not (fig. 1). The results of the 2 rounds of voting on the 34 recommendations are presented in table 1.

Delphi results.
| No. | Recommendation | 1st round% agreement | 2nd round% agreement | 2nd round% disagreement | Final result |
|---|---|---|---|---|---|
| BLOCK A - ON PREFERENCES FOR TOPICAL ACNE TREATMENT | |||||
| 1 | What I value most when prescribing a topical treatment is its EFFICACY | 95.50% | * | CONSENSUS | |
| 2 | What I value most when prescribing a topical treatment is its TOLERABILITY | 90.20% | * | CONSENSUS | |
| 3 | What I value most when prescribing a topical treatment is its SIMPLICITY in the ROUTINE/DOSAGE | 75.90% | 82.70% | MAJORITY | |
| 4 | Skin IRRITATION is a barrier to prescribing a topical treatment | 54.10% | 64.70% | NO CONSENSUS | |
| 5 | The WAITING TIME to obtain results is a barrier to prescribing a topical treatment | 43.60% | 47.40% | NO CONSENSUS | |
| 6 | PHOTOSENSITIVITY is a barrier to prescribing a topical treatment | 35.30% | 30.10% | NO CONSENSUS | |
| BLOCK B - ON SKIN IRRITATION AND TOPICAL ACNE TREATMENT WITH RETINOIDS | |||||
| 7 | I consider irritation an EXPECTED reaction at the start of treatment and not an undesirable side effect | 94.70% | * | CONSENSUS | |
| 8 | Mild and controllable skin irritation occurs FREQUENTLY at the BEGINNING of treatment | 98.50% | * | CONSENSUS | |
| 9 | Skin irritation tends to DECREASE gradually over time | 96.20% | * | CONSENSUS | |
| 10 | It is important to TELL the patient that temporary irritation is normal and expected, and they should not discontinue treatment because of it | 98.50% | * | CONSENSUS | |
| 11 | Skin irritation can be PREVENTED and/or REDUCED by following proper guidelines/recommendations for treatment application | 97.00% | * | CONSENSUS | |
| 12 | Patients who PROPERLY FOLLOW the application recommendations/guidelines tend to have fewer skin irritation problems than those who DO NOT | 94.70% | * | CONSENSUS | |
| BLOCK C - ON RECOMMENDATIONS/GUIDELINES TO PREVENT/REDUCE SKIN IRRITATION IN TOPICAL ACNE TREATMENT WITH RETINOIDS | |||||
| 13 | Correctly applying the topical retinoid at night helps PREVENT and/or REDUCE skin irritation | 91.00% | * | CONSENSUS | |
| 14 | WASHING THE FACE with specific products in the morning to remove retinoid residues helps PREVENT and/or REDUCE skin irritation | 79.70% | 87.97% | CONSENSUS | |
| 15 | DRYING THE FACE “BY PATTING” (without rubbing) helps PREVENT and/or REDUCE skin irritation | 77.40% | 89.47% | CONSENSUS | |
| 16 | SPACING OUT topical retinoid applications helps PREVENT and/or REDUCE skin irritation | 99.20% | * | CONSENSUS | |
| 17 | Combining treatment with specific non-comedogenic moisturizers with SPF helps PREVENT and/or REDUCE skin irritation | 94.00% | * | CONSENSUS | |
| 18 | The wash-off technique (applying treatment, waiting 30-60 minutes, and washing the face with a specific product) helps PREVENT and/or REDUCE skin irritation | 60.90% | 75.94% | MAJORITY | |
| 19 | I find the following standard administration protocol for starting topical retinoid treatment for acne to be correct - SEE FIGURE 3 | 88.00% | * | CONSENSUS | |
| BLOCK D - ON EXTREME WEATHER CONDITIONS AND SKIN IRRITATION AND TOPICAL ACNE TREATMENT WITH RETINOIDS | |||||
| 20 | It is preferable to START topical retinoid treatment for acne when the WEATHER IS NOT EXTREME | 63.20% | 67.67% | NO CONSENSUS | |
| 21 | The time of year DOES NOT MATTER when starting topical retinoid treatment for acne | 39.80% | 39.85% | NO CONSENSUS | |
| 22 | I prefer to INTERRUPT topical retinoid treatment during periods of EXTREME WEATHER in ANY patient | 14.30% | 88.72% | CONSENSUS | |
| 23 | In PATIENTS WHO HAVE BEEN ON THERAPY FOR A SHORT PERIOD OF TIME, I prefer to DISCONTINUE topical retinoid treatment during periods of EXTREME WEATHER | 15.80% | 6.80% | 81.95% | MAJORITY |
| 24 | In PATIENTS WHOSE ACNE IS ALREADY UNDER CONTROL, I suggest spacing out treatment when it coincides with periods of EXTREME WEATHER | 57.90% | 78.20% | MAJORITY | |
| 25 | If the PATIENT TOLERATES topical retinoids WELL and HAS NO IRRITATION, it is NOT necessary to DISCONTINUE treatment at any time of year | 92.50% | * | CONSENSUS | |
| 26 | During extreme weather conditions, I prefer my patients to SPACE OUT the applications of topical retinoids | 43.60% | 59.40% | NO CONSENSUS | |
| 27 | By following good application guidelines and recommendations, I consider that it is NOT NECESSARY to DISCONTINUE topical retinoid treatment during periods of extreme weather (intense cold or high sun exposure) | 88.70% | * | CONSENSUS | |
| 28 | With good sun protection (SPF 30-50), topical retinoids can be prescribed at ANY time of year | 87.20% | * | CONSENSUS | |
| 29 | Good sun protection (SPF 30-50) helps PREVENT and/or REDUCE SUN EXPOSURE IRRITATION in skin treated with topical retinoids | 92.50% | * | CONSENSUS | |
| 30 | Good MOISTURIZATION WITH SPF with specific non-comedogenic products helps PREVENT and/or REDUCE irritation during periods of intense cold | 97.00% | * | CONSENSUS | |
| 31 | PROTECTING THE SKIN WITH APPROPRIATE CLOTHING (long sleeves, hats, etc.) during periods of EXTREME WEATHER helps PREVENT and/or REDUCE irritation in skin treated with topical retinoids | 86.50% | * | CONSENSUS | |
| 32 | I avoid topical retinoid treatment in patients with FAIR SKIN TYPES during periods of high sun exposure | 25.60% | 12.80% | 81.20% | MAJORITY |
| 33 | Irritation due to photosensitization from topical retinoids is a VERY COMMON issue in my clinical practice | 21.10% | 9.02% | 80.50% | MAJORITY |
| 34 | It is important to REAPPLY sun protection if spending a long time outside, sweating excessively, or if the patient showers/bathes | 94.70% | * | CONSENSUS | |
Criteria for consensus on each recommendation were established if 85% or more of the group members indicated their agreement with the statement in either one of the 2 rounds and the criteria for majority consensus if 70% or more of the participants indicated their agreement with the recommendation in either one of the 2 rounds of voting.
When prescribing a topical treatment for facial and truncal acne, what experts value most is its efficacy and tolerability, with a 95.5% and 90.2% level of agreement respectively reached in the 1st round. Simplicity in the routine/dosage achieved a 75.9% level of agreement in the 1st round and majority consensus in the 2nd round with a 82.7% level of agreement.
Recommendation #4. Skin irritation is a barrier to prescribing a topical treatment.
Since only 64.7% of participants agreed with this statement in the 2nd round, it did not reach consensus. That skin irritation is a barrier to prescribing a topical treatment is a debatable and nuanced issue, as experts consider it a limiting factor only if appropriate measures to prevent or treat irritation are not taken, such as prescribing specific non-comedogenic moisturizers or spacing out applications if necessary. With proper precautions, skin irritation should not be an obstacle to prescribing topical retinoids for facial or truncal acne.
Recommendation #5. The waiting time to obtain results is a barrier to prescribing a topical treatment.
This statement received a <50% (47.10%) level of agreement in the 2nd round, and was, therefore, unable to reach consensus. The lack of agreement on this issue created some controversy within the group, as–a priori–the waiting time to see the first results was considered a relevant variable since patients usually prefer quick results. Any retinoid (whether oral or topical) takes time before the first results are noticeable, being a common thing for oral retinoids to cause an initial worsening of acne within the first weeks of treatment.18 One expert recommended starting with topical—before oral—retinoid treatment to avoid the usual initial worsening associated with oral retinoids.
There are patients for whom topical retinoid treatment would be indicated regardless of the time it takes to achieve results, such as patients who do not meet criteria for oral treatment, patients who need combined therapies (oral and topical), and those requiring maintenance with topical retinoids after finishing oral retinoid treatment.
Recommendation #6. Photosensitivity is a barrier to prescribing a topical treatment.
With only 30.10% agreement in the 2nd round, this statement received the lowest level of agreement of all consensus statements. It is well-known that sun exposure should be avoided while on topical retinoids,7 which is why it was particularly notable that there was no agreement on this issue. After analyzing the results, the expert committee explained this lack of agreement by considering that photosensitivity is not a barrier per se since there are easily accessible and applicable tools (photoprotectors) for patients. None of the experts, from the Iberian Peninsula or the Balearic and Canary Islands, would refrain from prescribing a topical treatment due to photosensitivity. Even in some cases with a high risk of photosensitivity, topical retinoid treatment might be preferred over full-dose oral retinoids, which can have more side effects of irritation and photosensitivity than a properly applied topical treatment.
Block B. On skin irritation and topical acne treatment with retinoidsThe 6 recommendations voted in this block reached consensus (level of agreement ≥ 85%) in the 1st round, making it the block with the highest level of agreement among all those evaluated.
Recommendation #8. Mild and controllable skin irritation frequently occurs at the beginning of treatment.
Recommendation #10. It is important to tell the patient that temporary irritation is normal and expected and, therefore, treatment should not be discontinued.
These 2 recommendations achieved consensus with a 98.5% level of agreement. Consensus was unanimous regarding irritation being associated with topical retinoid treatment as an expected, mild, and controllable side effect at the beginning of treatment that tends to decrease over time. The entire expert committee agreed on the importance of explaining how retinoids work to avoid treatment discontinuation due to a lack of results within the first few days of treatment or poor tolerability.
Recommendation #7. I consider that irritation is an expected reaction at the start of treatment and not an undesirable side effect.
Recommendation #12. Patients who follow the application recommendations/guidelines properly tend to have fewer skin irritation problems than those who do not.
These 2 issues reached consensus with a 94.7% level of agreement in the 1st round. The experts showed a high level of agreement on the importance of explaining patients that if they apply the guidelines/recommendations properly, they will have fewer tolerability issues, and that they should not discontinue treatment despite initial irritation since it is not an undesirable side effect (except for very sensitive skin).
Recommendation #11. Skin irritation can be prevented and/or reduced by following correct application guidelines/recommendations.
A total of 97% of participants considered that skin irritation treated with topical retinoids can be prevented/reduced if the proper guidelines/recommendations are followed. The expert committee summarized the main recommendations in Figure 2.
Block C. On recommendations/guidelines to prevent/reduce skin irritation in topical acne treatment with retinoids
In this block, a total of 7 recommendations were evaluated, 4 of which reached consensus in the 1st round. Specifically, recommendation #16, “spacing the applications of topical retinoids helps prevent and/or reduce skin irritation,” with a 99.2% level of agreement, was the recommendation that obtained the highest level of agreement among all the issues on which votes were cast.
Recommendation #13. Applying topical retinoid correctly at night helps prevent and/or reduce skin irritation.
Recommendation #17. Combining treatment with specific non-comedogenic moisturizers and SPF helps prevent and/or reduce skin irritation.
These 2 recommendations achieved broad consensus, with 91% and 94% levels of agreement, respectively in the 1st round as strategies to improve the tolerability of topical retinoid treatment.
Recommendation #14. Washing the face with specific products in the morning to remove retinoid residues helps prevent and/or reduce skin irritation.
Recommendation #15. Drying the skin by patting (without rubbing) helps prevent and/or reduce skin irritation.
These 2 recommendations reached consensus in the 2nd round with a nearly 90% level of agreement in both cases (see detailed results in table 1). The expert committee considers these 2 measures of paramount importance regarding good tolerability associated with topical retinoids: washing the face in the morning to remove the residues of the treatment applied the night before with specific non-comedogenic products and doing so carefully without rubbing the skin when drying.
Recommendation #18. The wash-off technique (applying treatment, waiting 30 to 60minutes, and washing the face with a specific product) is a measure that helps prevent and/or reduce skin irritation.
In the 2nd round, “the wash-off technique (applying treatment, waiting 30 to 60minutes, and washing the face with a specific product) is a measure that helps prevent and/or reduce skin irritation” that obtained a majority level of agreement with 76%. Although this technique can slow down the process of applying treatment, it is an interesting technique for very sensitive skins, especially within the first few days of treatment.
Recommendation #19. I find the following standard administration protocol for initiating topical retinoid treatment for acne to be correct (see figure 2).
A total of 88% of voters found the standard administration protocol for initiating topical retinoid treatment for acne presented in Figure 3 to be correct in the 1st round. Having a validated schedule to start a topical retinoid treatment was a requirement that the expert committee considered necessary when sharing these recommendations with other medical professionals.
Block D. On extreme weather conditions and skin irritation and topical acne treatment with retinoids
With 15 recommendations, this block was the most extensive of the 4 and generally obtained the lowest level of agreement: 8 issues reached consensus (7 in the 1st round and 1 in the 2nd round), 4 issues achieved a majority consensus, and 3 did not reach any levels of agreement.
Recommendation #20. It is preferable to START a topical retinoid treatment for acne when the weather is not extreme.
Recommendation #21. The time of year does not matter when starting a topical retinoid treatment for acne.
Neither of these 2 issues, with 67.7% and 39.8% levels of agreement, respectively, in the 2nd round, reached consensus or a majority consensus either.
Starting topical retinoid treatment during extreme weather conditions, i.e., periods of high sun exposure (summer months in the Iberian Peninsula) or intense cold (winter months in the Iberian Peninsula), were the issues that generated the most controversy within this block. The expert group concluded that, considering that the use of topical retinoids in extreme weather conditions is closely related to irritation (cold) and photosensitization (heat/sun), it seems logical that these issues did not reach consensus (which is consistent with recommendations #4 and #6 from block A, which also did not reach consensus).
Recommendation #26. During extreme weather conditions, I prefer my patients to space out the applications of topical retinoids.
This recommendation received a 59.4% level of agreement in the 2nd round, not reaching a majority consensus or consensus for that matter. The expert committee clarified that the need to space out applications does not depend so much on the time of year but on the tolerability and the phase of the treatment the patient is in. Spacing out applications is a recommended and widely used measure at the beginning of the treatment or when the patient experiences a high level of irritation, regardless of the weather.
Recommendation #32. I avoid topical retinoid treatment in patients with fair skin types during periods of high sun exposure.
A majority disagreement was reached (81.2% in the 2nd round) that, in patients with fair skin phototypes, it is not necessary to avoid topical retinoid treatment during periods of high sun exposure. In fact, although it can occur in any patient, post-inflammatory hyperpigmentation in acne patients is more common in darker skin types.19 The expert committee emphasized that in any patient, the proper application of photoprotection provides protection regardless of the patient's skin type.
Recommendation #33. Irritation due to photosensitization by topical retinoids is a very common issue in my clinical practice.
There was a majority disagreement (80.50% in the 2nd round of voting) that irritation due to photosensitization induced by topical retinoids is a very common issue in the dermatologists’ office. Some experts acknowledged not having seen any patients with photosensitization due to topical retinoids, but some with photosensitization due to oral retinoids.
DiscussionThis document presents a series of strategies and practical recommendations on how to reduce or prevent tolerability issues of topical retinoids to treat facial and truncal acne. The Delphi methodology was followed and followed by a large group of dermatologists from Spain and Portugal, thereby reinforcing the validity of the recommendations.
Notably, a high level of agreement was reached on the recommendations (fig. 1): 82.3% of them, 28 out of 34, achieved some level of agreement (22 reached consensus with a ≥ 85% level of agreement and 6 reached a majority consensus with a ≥ 70% level of agreement).
Consensus was almost unanimous (94.7%) that patients who properly follow the application recommendations/guidelines (fig. 2) tend to have fewer tolerability issues than those who do not. These recommendations are simple and very easy to apply, so it is essential to disseminate them widely both to the medical community and to patients.
Based on the consensus results and its own experience, the expert committee concluded that topical retinoid-related skin irritation is an expected, mild, and controllable reaction if correct prevention and management guidelines are followed. Therefore, it should not be a reason to discontinue treatment, which is why the expert committee emphasized the importance of dedicating part of the consultation to explaining the various strategies to the patient and recommended providing supporting materials for the patient.
With this consensus, the expert committee fulfills the objective of this project: to provide recommendations endorsed by a large panel of dermatologists, helping other health care professionals treating acne improve topical retinoid treatments for facial and truncal acne.
FundingGalderma has collaborated in the funding of the project. However, this sponsoring laboratory did not participate in the drafting of the article.
Conflicts of interestNone of the authors declared any conflicts of interest on the topics covered in this article, which they have defended solely based on their clinical experience.
Dr. Alexander Catarino has received support from Galderma to attend the AEDV 2021 congress. Dr. Cristina Eguren has received support for attending meetings and/or travel expenses from Galderma. Dr. Cristina Eguren is president of DERMUS (Association of Private Dermatology Clinics), a member of the AEDV (Spanish Association of Dermatology and Venereology) board of trustees, and a member of the international council of dermatologists for L’Oreal Paris. Dr. M. Isabel Hernández Jurado declared to have received payments or fees for lectures, presentations, speaker bureaus, manuscript drafting, or educational events. Dr. Montse Salleras has received consulting fees from Galderma, Lilly, LEO Pharma, and ISDIN; payments or fees for lectures, presentations, speaker bureaus, manuscript drafting, or educational events from Galderma, Lilly, LEO Pharma; payment for expert testimony from Galderma and ISDIN; support for attending meetings and/or travel expenses from Lilly, LEO Pharma, ABBVIE, UCB Pharma, Almirall, Janssen, and ISDIN. Dr. Susanna Nogueras has received consulting fees from Galderma. Dr. Nayra Merino has received payments or fees for lectures, presentations, speaker bureaus, manuscript drafting, or educational events from Galderma, as well as medical materials from Galderma.


