



High-grade anal intraepithelial neoplasia (AIN) is considered a precursor to anal cancer. Its incidence has increased in specific risk populations, especially persons infected by the human immunodeficiency virus (HIV) and men who have sex with men (MSM).1
Human papillomavirus (HPV) has been shown to play a key pathogenic role in anal cancer (up to 93% of cases). In fact, the frequency of oncogenic genotypes 16 and 18 has increased significantly in both high-grade AIN and anal carcinoma.1
Although the natural course of AIN is unknown and recurrence rates of up to 29% have been reported, the condition sometimes progresses to infiltrating forms, especially in older HIV-infected patients with CD4 T-lymphocyte counts <200cells/μL.2
There is no definitive protocol for screening of AIN, in part because of a lack of data on the role of screening in reducing the morbidity and mortality of anal cancer. Most authors base their reports on the program proposed by Chin-Hong and Palefsky,3 which does not take into account HPV genotyping as an initial screening test.
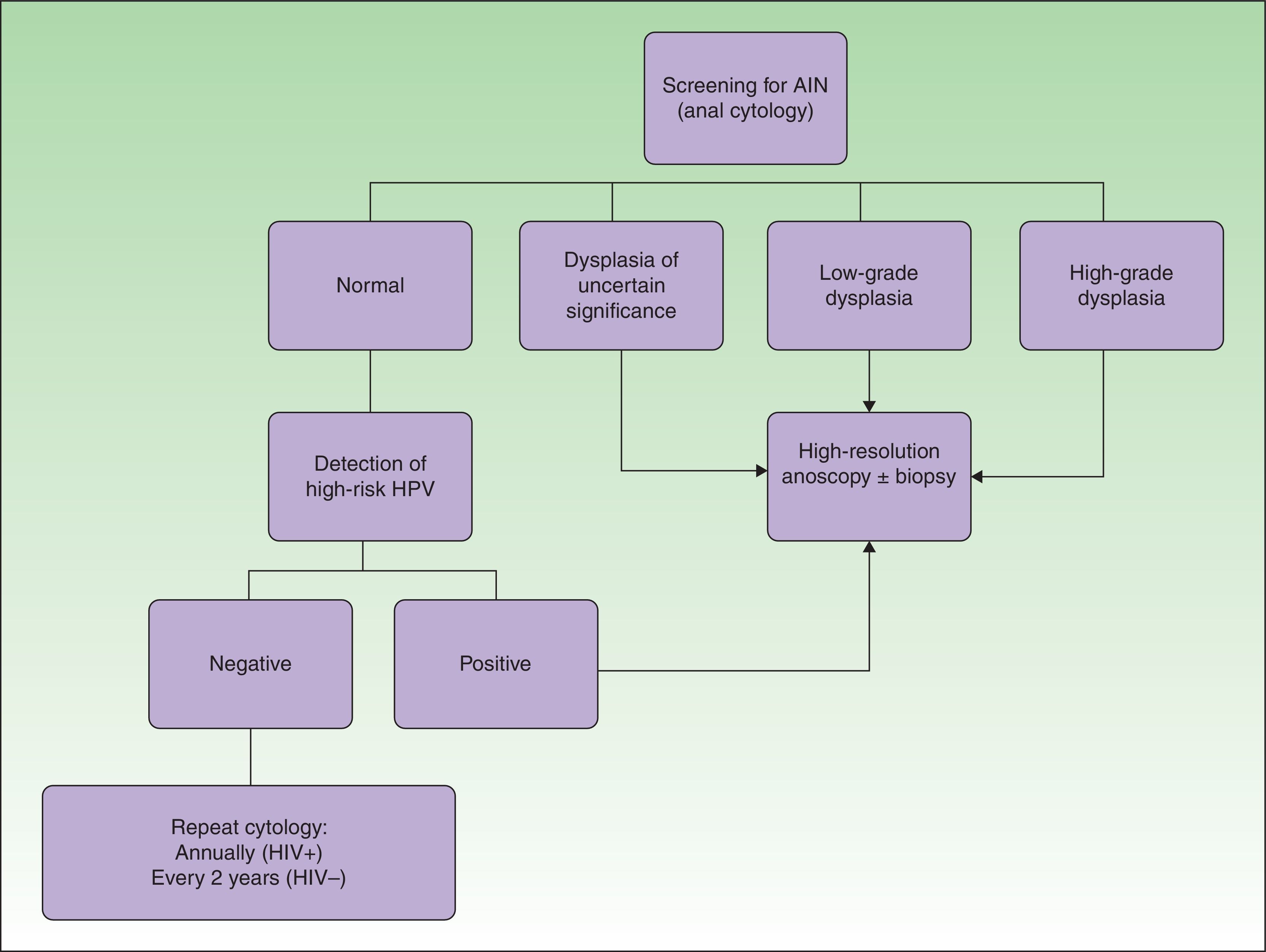
Screening for AIN is based on the combination of anal cytology and high-resolution anoscopy, as in screening for cervical cancer. However, it is important to remember that anal cytology can lead high-grade AIN to be underdiagnosed, especially in immunodepressed patients (up to 52.7% cases according to Botes et al.4).
Hybrid capture assay and HPV genotyping tests were recently proposed as complementary tools in screening for AIN. Risk genotypes are detected using microplate DNA hybridization assay and subsequent chemiluminescence signal amplification for the qualitative detection of different genotypes of low- and high-risk HPV. This technique is supported by several correlation studies (performed specifically in HIV-infected patients) that compare the findings of both diagnostic methods (anal cytology and detection of HPV), with a strong association between high-grade dysplasia and infection by multiple high-risk HPV genotypes.2
Detection of high-risk genotypes could prove to be essential in high-risk populations, such as HIV-infected patients and MSM, in whom anal cytology does not show dysplasia to be present. In these cases, a meticulous examination of the anal canal should be performed using high-resolution anoscopy that enables suspected high-grade AIN lesions to be identified and biopsied (Fig. 1).
Therefore, the latest trends point to HPV genotyping as the most sensitive and specific tool when screening for AIN.5 Nevertheless, it is necessary to perform sensitivity and cost-effectiveness studies to compare the various diagnostic procedures used in screening with anoscopy-guided biopsy, which continues to be the definitive confirmatory diagnostic test.
Please cite this article as: Padilla-España L, Millán Cayetano JF, García Montero P. Detection of Oncogenic Human Papillomavirus Genotypes: A Useful Screening Tool for High-Grade Anal Intraepithelial Neoplasia. Actas Dermosifiliogr. 2015;106:835–836.


