





Risankizumab – a humanized monoclonal antibody that targets the p19 subunit of IL-23 – has been recently approved to treat moderate-to-severe plaque psoriasis. Real-world data based on a representative pool of patients are currently lacking.
ObjectiveTo assess the mid- and long-term safety and efficacy profile of risankizumab in patients with moderate-to-severe psoriasis in the routine clinical practice.
MethodsThis was a retrospective and multicenter study of consecutive psoriatic patients on risankizumab from April 2020 through November 2022. The primary endpoint was the number of patients who achieved a 100% improvement in their Psoriasis Area and Severity Index (PASI) (PASI100) on week 52.
ResultsA total of 510 patients, 198 (38.8%) women and 312 (61.2%) men were included in the study. The mean age was 51.7±14.4 years. A total of 227 (44.5%) study participants were obese (body mass index [BMI] >30kg/m2). The mean baseline PASI score was 11.4±7.2, and the rate of patients who achieved PASI100 on week 52, 67.0%. Throughout the study follow-up, 21%, 50.0%, 59.0%, and 66% of the patients achieved PASI100 on weeks 4, 16, 24, and 40, respectively. The number of patients who achieved a PASI ≤2 was greater in the group with a BMI ≤30kg/m2 on weeks 4 (P=.04), 16 (P=.001), and 52 (P=.002). A statistically significantly greater number of patients achieved PASI100 in the treatment-naïve group on weeks 16 and 52 (P=.001 each, respectively). On week 16 a significantly lower number of participants achieved PASI100 in the group with psoriatic arthropathy (P=.04). Among the overall study sample, 22 (4.3%) patients reported some type of adverse event and 20 (3.9%) discontinued treatment.
ConclusionsRisankizumab proved to be a safe and effective therapy for patients with moderate-to-severe psoriasis in the routine clinical practice.
Risankizumab es un anticuerpo monoclonal humanizado que se dirige a la subunidad p19 de IL-23, recientemente aprobado para el tratamiento de la psoriasis en placas moderada a grave. Actualmente faltan datos del mundo real basados en una muestra representativa de pacientes.
ObjetivoEvaluar la eficacia y la seguridad a medio y a largo plazo del risankizumab en pacientes con psoriasis moderada a grave en la práctica clínica habitual.
MétodosEstudio retrospectivo y multicéntrico realizado en pacientes consecutivos con psoriasis que recibieron tratamiento con risankizumab desde abril de 2020 hasta noviembre de 2022. El criterio de valoración principal fue la proporción de pacientes que alcanzaron una mejora en el Índice de Área y Severidad de la Psoriasis (Psoriasis Area and Severity Index [PASI]) del 100% (PASI100) en la semana 52.
ResultadosSe incluyeron en el estudio un total de 510 pacientes, 198 (38,8%) mujeres y 312 (61,2%) hombres. La edad media fue de 51,7±14,4 años, y 227 (44,5%) sujetos eran obesos (índice de masa corporal [IMC]>30kg/m2). La puntuación media del PASI basal fue de 11,4±7,2. La proporción de pacientes que alcanzaron PASI100 en la semana 52 fue del 67,0%. A lo largo del seguimiento del estudio, el 21%, el 50,0%, el 59,0% y el 66% de los pacientes alcanzaron un PASI100 en las semanas 4, 16, 24 y 40, respectivamente. La proporción de pacientes que alcanzaron un PASI≤2 fue mayor en el grupo con un IMC≤30kg/m2 en la semana 4 (p=0,04), la semana 16 (p=0,001) y la semana 52 (p=0,002). Una proporción estadísticamente significativa mayor de pacientes alcanzó un PASI100 en el grupo sin tratamiento previo en la semana 16 y a la semana 52 (p=0,001 en cada una, respectivamente). En la semana 16, una proporción significativamente menor de sujetos alcanzó un PASI100 en el grupo con artropatía psoriásica (p=0,04). Entre la muestra total del estudio, 22 (4,3%) pacientes reportaron algún tipo de evento adverso y 20 (3,9%) abandonaron o se retiraron del tratamiento.
ConclusionesRisankizumab fue un tratamiento efectivo y seguro para pacientes con psoriasis moderada a grave en la práctica clínica.
Psoriasis is a chronic, immune-mediated inflammatory, and multifactorial skin disease described worldwide, which can affect people of any age, and lead to a substantial disease burden for individuals and health systems alike.1–3
Determining disease severity is an important but challenging issue that requires a combined assessment of clinical and patient-reported factors.4,5 The Psoriasis Area and Severity Index (PASI) is currently considered as the gold standard for assessing extensive psoriasis.4,6 Other objective tool to assess the severity of psoriasis is the body surface area (BSA).5,7
Although, to this date, psoriasis cannot be cured, different treatment options, aimed at minimizing its impact and preventing associated multimorbidities, are currently available.2,3
Biologics have dramatically changed the treatment paradigm of psoriasis.8,9 They have proven to be more effective than conventional therapies to treat mild-to-severe psoriasis.8–10 Biologics have been categorized based on their target into tumour necrosis factor inhibitors (anti-TNF), interleukin (IL)-12/23 inhibitors, IL-17 inhibitors, IL-17 receptor inhibitors, and IL-23 inhibitors.8,9
Among the currently available diverse biologic treatments, risankizumab (a humanized monoclonal antibody that targets p19 subunit of IL-23)11 was approved in 2019 by the U.S. Food and Drug Administration (FDA) and European Medical Agency (EMA) to treat moderate-to-severe plaque psoriasis.12
The safety and efficacy profile of risankizumab in patients with moderate-to-severe psoriasis, had previously been evaluated in four multicenter randomized clinical trials (UltIMMa-1, UltIMMa-2, IMMHANCE, and IMMVENT).13–15 The results of these clinical trials also confirm the good safety and efficacy profile of risankizumab in patients with moderate-to-severe psoriasis.13–15
Despite the good results reported by these 4 randomized clinical trials, their samples are not representative of the real world; which is much more heterogenous.
The safety and efficacy of risankizumab under real-world conditions was assessed in high-need psoriatic patients.16–20 Risankizumab provided rapidly improved clinical signs and relieved symptoms in these cohorts of patients with moderate-to-severe psoriasis.16–20
Due to limited evidence, there is this need to assess the clinical outcomes of risankizumab in the routine clinical practice.
The present article aimed to evaluate the mid- and long-term safety and efficacy of risankizumab in patients with moderate-to-severe psoriasis in the routine clinical practice, and the impact of different factors on treatment outcomes.
MethodsStudy designThis was a retrospective, multicenter, observational, and non-interventional study of consecutive psoriatic patients on risankizumab from April 2020 through November 2022.
The study protocol was approved by Hospital de Manises research and ethics committee, which deed the patient's prior written informed consent unnecessary.
The study protocol complied with the principles established in the Declaration of Helsinki and the Good Clinical Practice/International Council for Harmonization Guidelines.
ParticipantsPatients aged ≥18 years old with a clinical diagnosis of psoriasis on risankizumab from April 2020 through November 2022.
OutcomesThe primary endpoint was the number of patients who achieved a PASI of 100% (PASI100) on week 52.
The secondary outcomes included the mean PASI score on week 52, the number of patients who achieved PASI100 on weeks 4, 16, 24, and 40, and the incidence of adverse events.
Additionally, the impact of different factors, including obesity [defined according to the World Health Organization classification as a body mass index (BMI) >30kg/m2],21 the presence of psoriatic arthritis, previous treatment status (naïve vs previously treated); and previous biologic drugs used were also evaluated.
Statistical analysisA standard statistical analysis was performed using SPSS statistical software version 28 (IBM SPSS Statistics, IL, United States).
Descriptive statistics (percentage) and mean±standard deviation (SD) were used, as appropriate.
Data were tested for normal distribution using the Shapiro–Wilk test.
The one-way ANOVA test was used to assess inter-group differences.
Categorical variables were compared using the chi-square test and Fisher's exact test, as required.
P values <0.05 were considered statistically significant.
ResultsBaseline demographics and clinical characteristicsA total of 510 patients, 198 (38.8%) women and 312 (61.2%) men were included in the study. Mean age was 51.7±14.4 years and 227 (44.5%) study participants were obese (BMI >30kg/m2).
Among the overall study population, 476 (93.3%) were diagnosed with vulgar psoriasis.
The mean course of the disease was 21.0±13.7 years and the mean PASI score, 11.4±7.2.
A total of 396 patients (77.6%) had previous been on conventional systemic treatment and 418 (81.9%) on biologic therapies.
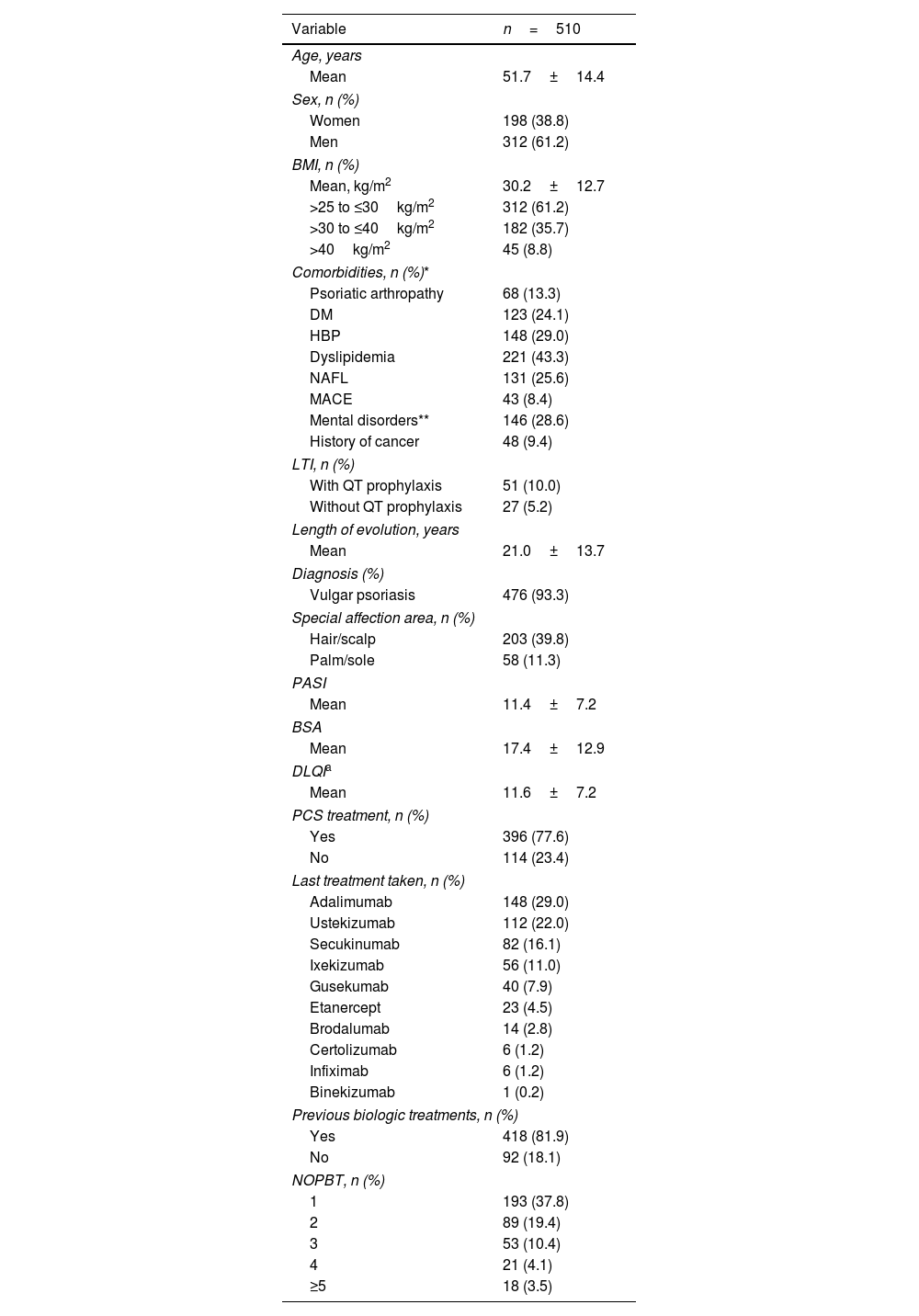
Table 1 illustrates the main clinical and demographic characteristics of the study sample.
Baseline demographic and clinical characteristics.
| Variable | n=510 |
|---|---|
| Age, years | |
| Mean | 51.7±14.4 |
| Sex, n (%) | |
| Women | 198 (38.8) |
| Men | 312 (61.2) |
| BMI, n (%) | |
| Mean, kg/m2 | 30.2±12.7 |
| >25 to ≤30kg/m2 | 312 (61.2) |
| >30 to ≤40kg/m2 | 182 (35.7) |
| >40kg/m2 | 45 (8.8) |
| Comorbidities, n (%)* | |
| Psoriatic arthropathy | 68 (13.3) |
| DM | 123 (24.1) |
| HBP | 148 (29.0) |
| Dyslipidemia | 221 (43.3) |
| NAFL | 131 (25.6) |
| MACE | 43 (8.4) |
| Mental disorders** | 146 (28.6) |
| History of cancer | 48 (9.4) |
| LTI, n (%) | |
| With QT prophylaxis | 51 (10.0) |
| Without QT prophylaxis | 27 (5.2) |
| Length of evolution, years | |
| Mean | 21.0±13.7 |
| Diagnosis (%) | |
| Vulgar psoriasis | 476 (93.3) |
| Special affection area, n (%) | |
| Hair/scalp | 203 (39.8) |
| Palm/sole | 58 (11.3) |
| PASI | |
| Mean | 11.4±7.2 |
| BSA | |
| Mean | 17.4±12.9 |
| DLQIa | |
| Mean | 11.6±7.2 |
| PCS treatment, n (%) | |
| Yes | 396 (77.6) |
| No | 114 (23.4) |
| Last treatment taken, n (%) | |
| Adalimumab | 148 (29.0) |
| Ustekizumab | 112 (22.0) |
| Secukinumab | 82 (16.1) |
| Ixekizumab | 56 (11.0) |
| Gusekumab | 40 (7.9) |
| Etanercept | 23 (4.5) |
| Brodalumab | 14 (2.8) |
| Certolizumab | 6 (1.2) |
| Infiximab | 6 (1.2) |
| Binekizumab | 1 (0.2) |
| Previous biologic treatments, n (%) | |
| Yes | 418 (81.9) |
| No | 92 (18.1) |
| NOPBT, n (%) | |
| 1 | 193 (37.8) |
| 2 | 89 (19.4) |
| 3 | 53 (10.4) |
| 4 | 21 (4.1) |
| ≥5 | 18 (3.5) |
DM: diabetes mellitus; HBP: high blood pressure; MACE: major adverse cardiovascular events; NAFL: nonalcoholic fatty liver; LTI: latent tuberculosis infection; QT: chemotherapy; PASI: Psoriasis Area and Severity Index; BSA: body surface area; DLQI: Dermatology Life Quality Index; PCS: previous conventional systemic; NOPBT: number of previous biologic treatments.
The percentage of patients who achieved PASI100 on week 52 was 67.0% (Fig. 1).
 score.")
A total of 21%, 50.0%, 59.0%, and 66% of the patients achieved PASI100 on weeks 4, 16, 24, and 40, respectively, at the follow-up.
The mean PASI score significantly dropped from 11.4±7.2 at baseline to 4.0±5.0; 1.6±3.5, 1.2±3.1, 0.8±2.0, and 0.6±1.7 on weeks 4, 16, 24, 40, and 52, respectively; P=.001 each, respectively (Fig. 2).
Factors associated with PASSIBody mass index score achieved at the follow-up. Vertical bars show the standard deviation.")
To assess the effect obesity had on the clinical outcomes, the study population was categorized based on their BMI into two groups: obese (BMI >30kg/m2) vs no-obese (BMI ≤30kg/m2).22
Although the number of subjects who achieved PASI100 at the follow-up was similar in both groups (Fig. 3A), a statistically significant greater number of patients achieved a PASI ≤2 on week 2 (P=.04), week 16 (P=.001), and week 52 (P=.002) in the group with a BMI ≤30kg/m2 (Fig. 3B).
Treatment status (treatment-naïve vs previously treated) improvement of 100% (PASI100) (A) and a PASI <2 (B) based on their body mass index (BMI). BMI: body mass index; PASI: Psoriasis Area and Severity Index.")
A statistically significantly greater number of patients achieved PASI100 in the treatment-naïve group on weeks 16 and 52 (P=.001 each, respectively) (Fig. 4A).
 improvement of 100% (PASI100) (A) and a PASI <2 (B) based on their treatment status (treatment-naïve vs previously treated).")
Similarly, significantly more patients achieved a PASI score <2 in the treatment-naïve group on weeks 16 and 52 (P=.008 and P=.01, respectively) (Fig. 4B).
Psoriatic arthropathyThe study sample was categorized into two groups: patients with and without psoriatic arthropathy.
A significantly greater number of participants achieved PASI100 in the group without psoriatic arthropathy on week 16 (P=.04) (Figure S1A, supplementary data).
Regarding the participants who achieved a PASI score <2, the number was significantly greater in the group without psoriatic arthropathy on weeks 4 (P=.03), 16 (P=.001), and 24 (P=.04) (Figure S1B, supplementary data).
Biologic therapyThe study sample was categorized based on the type of biologic therapy received in patients previously on anti-TNF, anti-IL-12/-23, anti-IL-17, or anti-IL-23.
The mean baseline PASI score was significantly lower in all four groups at all time periods measured, with no statistically significant differences being reported among them (Figure S2, supplementary data).
Figure S3 illustrates the number of patients who achieved PASI100 or a PASI <2 based on the previous biologic therapies received.
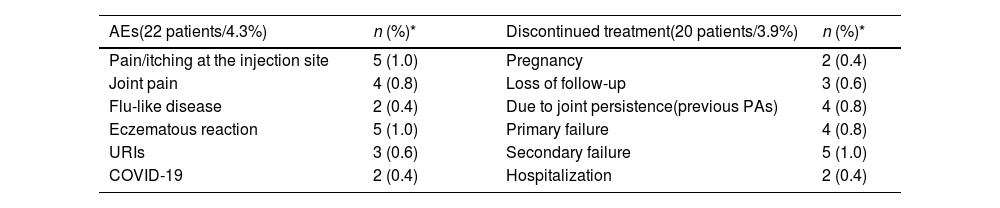
SafetyAmong the overall study sample, 22 (4.3%) patients reported some type of adverse event and 20 (3.9%) discontinued treatment (Table 2).
Incidence of adverse events throughout the study follow-up.
| AEs(22 patients/4.3%) | n (%)* | Discontinued treatment(20 patients/3.9%) | n (%)* | |
|---|---|---|---|---|
| Pain/itching at the injection site | 5 (1.0) | Pregnancy | 2 (0.4) | |
| Joint pain | 4 (0.8) | Loss of follow-up | 3 (0.6) | |
| Flu-like disease | 2 (0.4) | Due to joint persistence(previous PAs) | 4 (0.8) | |
| Eczematous reaction | 5 (1.0) | Primary failure | 4 (0.8) | |
| URIs | 3 (0.6) | Secondary failure | 5 (1.0) | |
| COVID-19 | 2 (0.4) | Hospitalization | 2 (0.4) |
URIs: upper respiratory tract infections; COVID-19: coronavirus disease 2019; PAs: psoriatic arthropathy.
The most widely reported adverse events was pain/itching at the injection site and eczematous reactions (5/22 each, respectively) (Table 2).
Regarding patients who discontinued treatment, the most frequent reasons for the discontinuation were secondary failure (5/20) and joint persistence (previous psoriatic arthropathy) and primary failure (5/20 each, respectively) (Table 2).
DiscussionNew advances in knowledge on the pathogenesis of psoriatic disease, in particular, the crucial role of IL-17/-23 axis,23,24 have led to the development of new therapeutic tools with selective action that have made it possible to achieve significant results in terms of efficacy, with an optimal safety profile too.9–20
The considerable number of biologics currently available8,9 make real-world studies necessary for clinicians to be able to individualize approaches for the patients.25
Based on data published in 2001, in Spain, the prevalence of psoriasis was 1.4%.26 However, the advent of biologic therapies has triggered significant changes in the treatment paradigm, since they have a better safety and efficacy profile vs previous treatments.8,9 The widespread use and acceptance of these new therapeutic options have led to better and more information on psoriasis, which has consequently meant an increase in its prevalence. In fact, according to the latest data published to date, the prevalence of psoriasis in Spain was estimated at 2.3%.27
This retrospective and multicenter study conducted on a Spanish cohort of 510 patients with moderate-to-severe psoriasis, assessed the safety and efficacy profile of risankizumab at a 52-week follow-up.
According to the results of the current study, risankizumab significantly reduced the baseline PASI score in all the time periods measured. Moreover, on week 52, 67%, 72.3%, 88%, and 93% of the patients achieved a PASI score=0 (PASI100), ≤1, ≤2, and ≤3, respectively.
Based on various factors, the efficacy of risankizumab was higher in patients with BMI <30kg/m2, treatment-naïve patients, and patients without psoriatic arthropathy. Additionally, in patients previously on biologics, risankizumab showed similar efficacy regardless of the biologics previously administered.
These results were consistent with those reported by the randomized clinical trials.13–15 It is difficult to make a direct comparison between our results and those from clinical trials since there are differences in some of the baseline parameters. For example, compared to UltIMMa-1, UltIMMa-2, IMMHANCE, and IMMVENT clinical trials,13–15 the PASI and BSA scores were lower in our study, while the patients from our study had received many more previous treatments.13–15
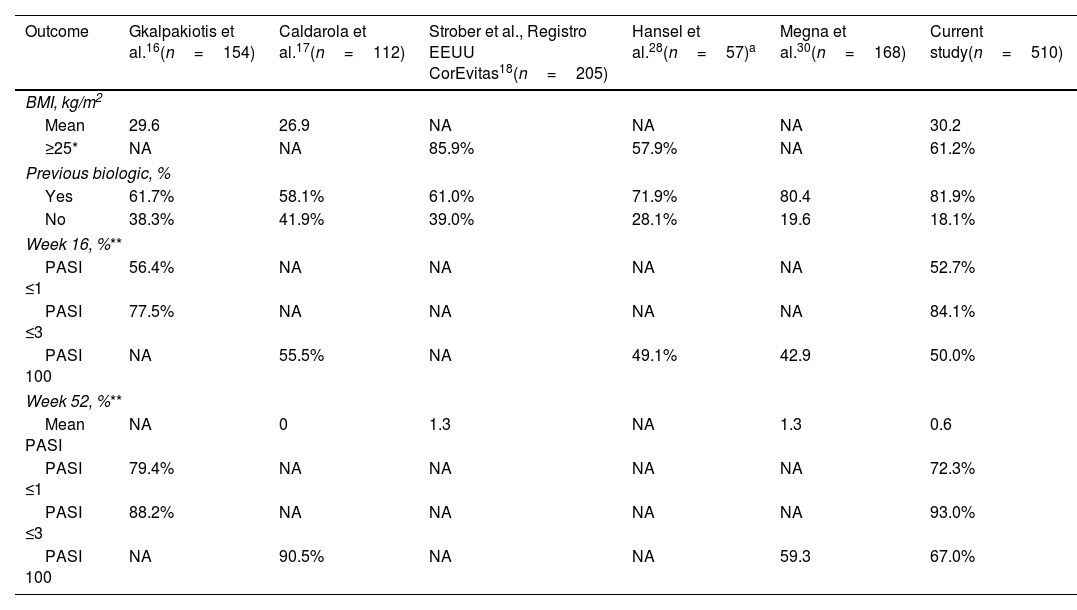
Regarding the comparison of the current study to those of larger real-world studies (Table 3), clinical outcomes were similar, although a greater number of our patients had been previously treated with other biologics.
A comparison of the clinical outcomes between the current study and the available evidence.
| Outcome | Gkalpakiotis et al.16(n=154) | Caldarola et al.17(n=112) | Strober et al., Registro EEUU CorEvitas18(n=205) | Hansel et al.28(n=57)a | Megna et al.30(n=168) | Current study(n=510) |
|---|---|---|---|---|---|---|
| BMI, kg/m2 | ||||||
| Mean | 29.6 | 26.9 | NA | NA | NA | 30.2 |
| ≥25* | NA | NA | 85.9% | 57.9% | NA | 61.2% |
| Previous biologic, % | ||||||
| Yes | 61.7% | 58.1% | 61.0% | 71.9% | 80.4 | 81.9% |
| No | 38.3% | 41.9% | 39.0% | 28.1% | 19.6 | 18.1% |
| Week 16, %** | ||||||
| PASI ≤1 | 56.4% | NA | NA | NA | NA | 52.7% |
| PASI ≤3 | 77.5% | NA | NA | NA | NA | 84.1% |
| PASI 100 | NA | 55.5% | NA | 49.1% | 42.9 | 50.0% |
| Week 52, %** | ||||||
| Mean PASI | NA | 0 | 1.3 | NA | 1.3 | 0.6 |
| PASI ≤1 | 79.4% | NA | NA | NA | NA | 72.3% |
| PASI ≤3 | 88.2% | NA | NA | NA | NA | 93.0% |
| PASI 100 | NA | 90.5% | NA | NA | 59.3 | 67.0% |
BMI: body mass index; PASI: Psoriasis Area and Severity Index; NA: not available.
Additionally, compared to Gkalpakiotis et al.16 and Caldarola et al.,17 our cohort has a greater BMI, which in view of our results could negatively impact results. In a multicenter and real-world study, Hansel et al.21,28 evaluated the safety and efficacy profile of risankizumab over a 16-28 and 52-week period21 in patients with psoriasis. As it is the case with former studies, the results of our study were like those reported by Hansel et al.21,28
Regarding the impact of BMI on the clinical outcomes, our study is consistent with Hansel et al.28 and Borroni et al.29 who reported that a higher BMI negatively impacted the efficacy of risankizumab. In contrast, the results of the current study differed from those reported by Gkalpakiotis et al.16, Caldarola et al.17, and Megna et al.30 who found that BMI did not affect the short- and long-term efficacy of risankizumab.
In the current study, the presence of psoriatic arthropathy negatively impacted the efficacy of risankizumab. Although no significant differences were reported in the number of patients who achieved PASI100 on week 52 between patients with or without psoriatic arthropathy, on week 16, many more patients without psoriatic arthropathy achieved PASI100.
The safety and efficacy profile of risankizumab in psoriatic arthritis patients was assessed in a double-blind and dose-ranging phase 2 trial.31 The results of this study found that the number of patients who achieved PASI100, among those treated with risankizumab, ranged between 33.3% and 5.6%, depending on the allocated dose.31
Regarding safety, this study did not see any unexpected adverse events. The incidence and type of adverse events was consistent with the evidence currently available.13–21,29–31
The main limitations of the current study are its retrospective design and the lack of a control group.
As far as we know, the main strength of this study is its sample size – the largest series to date (n=510) – of psoriatic patients on risankizumab in the routine clinical practice. Its other strength is its multicenter nature, including patients from different parts of Spain.
ConclusionsThe results of this study confirmed the good safety and efficacy profile of risankizumab in the routine clinical practice. The results of the study seemed to be impacted by the BMI (obese patients had worse outcomes), the presence of psoriatic arthritis, and previous therapies. Nevertheless, in these groups of patients with unfavourable characteristics the efficacy rates were quite good. Safety profile was, also, very good, with no unexpected adverse events being reported.
New prospective, multicenter, and controlled real-life studies are needed to assess the safety and efficacy profile of these biologic therapies.
FundingMedical writing service has been supported by the AEDV Psoriasis Working Group.
Conflicts of interestAntonio Martorell declared consultancy/speaker's fee, and/or travel expenses, and/or having participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Boehringer-Ingelheim, Celgene, Gebro, Janssen, LEO Pharma, Lilly, Novartis, Pfizer, Sandoz, Sanofi and UCB.
Alvaro González-Cantero has participated as an IP/SI and/or invited speaker, and/or advisor for Almirall, Janssen, Abbvie, UCB, Boehringer-Ingelheim, Lilly, Novartis, Amgen, BMS, and Sandoz.
Eva Vilarrasa declared consultancy and/or as a speaker's fees, and/or travel expenses, and/or having participated in clinical trials sponsored by Abbvie, Almirall, Amgen, Boehringer-Ingelheim, Bristol-Meyers Squibb, Celgene, Gebro, Isdin, Janssen, LEO Pharma, Lilly, Merck Serono, MSD, Novartis, Pfizer, Roche, Sandoz, Sanofi, and UCB.
Pablo de la Cueva declared having participated as an advisor, and/or investigator, and/or speaker for the following pharmaceutical companies: Abbvie, Almirall, BMS, Boehringer-Ingelheim, Celgene, Janssen Cilag, LEO Pharma, Lilly, MSD, Novartis, Novo Nordisk, Pfizer, Roche, Sanofi, and UCB.
Fernando Gallardo declared having received speaker and consultancy fees for his participation in courses, congresses, and/or research projects organized by Janssen, Abbvie, UCB, Amgen, Bristol, Lilly, Novartis, Almirall, and Leo Pharma.
José Manuel Carrascosa has participated as an IP/SI and/or invited speaker, and/or advisor for Almirall, Janssen, Abbvie, UCB, Boehringer-Ingelheim, Lilly, Novartis, Amgen, BMS, and Sandoz.
The remaining authors declared no conflicts of interest whatsoever.
Medical writing and Editorial assistant services have been provided by Ciencia y Deporte S.L.
The following are the supplementary data to this article:


