
A previously healthy man in his forties with no prior history of bites or stings presented with pruritic, erythematous plaques on his forearms that had developed 2 weeks earlier. His medical history included no medications or exposures associated with his skin condition. He had been previously treated with oral amoxicillin, with no response.
Physical examination revealed whitish-gray indurated plaques with surrounding erythema on the forearms (Fig. 1A). Laboratory tests including a complete blood count (no peripheral eosinophilia), serum electrolyte analysis, and bacterial and fungal cultures were negative. Skin biopsy showed spongiosis with subepidermal edema (Fig. 1B), perivascular eosinophilic infiltrate (Fig. 1C), diffuse interstitial inflammatory infiltrate with eosinophils and flame figures (Fig. 1D), and no evidence of vasculitis or foreign material.
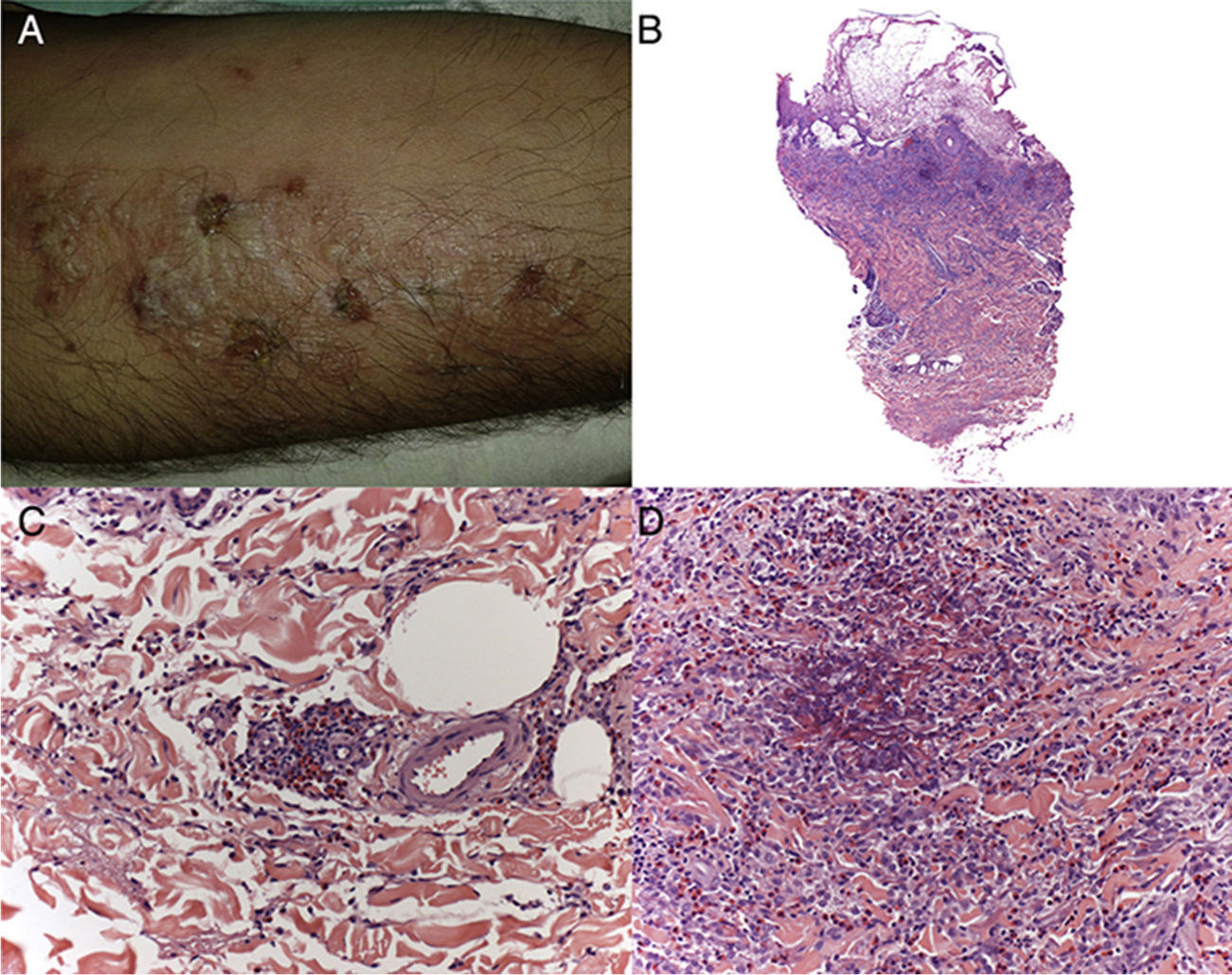
Based on the clinical and histological findings, a diagnosis of Wells syndrome (eosinophilic cellulitis) was established. The patient began treatment with systemic steroids (1mg/kg/d), which resulted in resolution of the lesions within 4 weeks. Subsequently, the dose of steroids was gradually reduced, and completely discontinued after 1 month.
While its initial clinical presentation can resemble that of cellulitis and several types of dermatitis, eosinophilic cellulitis can be distinguished from other dermatoses by its histological features (edema and dermal inflammatory infiltrate with eosinophils and flame figures) and the presence of whitish-gray, morphea-like, indurated plaques.



