



Angiolymphoid hyperplasia with eosinophilia (ALHE) is a benign vascular proliferation characterized by solitary or multiple angiomatous lesions. It is most common in young or middle-aged women, and the lesions typically affect the head and neck, showing a particular predilection for the periauricular region. The differential diagnosis in patients with ALHE is broad and includes both benign and malignant conditions. We report on a series of cases of periauricular ALHE in which ultrasound imaging revealed an hypervascular, pseudonodular and plaque-like morphology with clinical and histologic correlations. It also evidenced vascular communication between lesions that appeared to be separate on clinical examination. Familiarity with such ultrasound presentations could help to improve diagnostic accuracy and facilitate disease monitoring in patients with ALHE.
La hiperplasia angiolinfoide con eosinofilia (HALE) es una proliferación vascular benigna caracterizada por lesiones angiomatosas solitarias o múltiples, que se presentan más frecuentemente en mujeres jóvenes o de mediana edad, en cabeza y cuello, con predilección por la región periauricular. Esta enfermedad plantea un diagnóstico diferencial extenso, tanto con lesiones benignas como malignas, por lo que la posibilidad de tener una herramienta diagnóstica no invasiva como la ecografía puede ser de utilidad. Presentamos una serie de casos de HALE con morfología ecográfica «en placa pseudonodular hipervascular» de localización periauricular, con correlación clínica e histológica. Se demostró comunicación vascular ecográfica entre lesiones que parecían clínicamente separadas. El conocimiento de esta forma de presentación ecográfica podría contribuir a mejorar la precisión del diagnóstico y seguimiento evolutivo de estos casos.
Angiolymphoid hyperplasia with eosinophilia (ALHE) is a chronic benign vascular proliferation of uncertain origin, with an extensive differential diagnosis that includes other benign and malignant subcutaneous lesions.1
Color Doppler ultrasound is a noninvasive diagnostic technique that is increasingly common in dermatology.2–4 To date, there are 2 reports in the literature of the use of ultrasonography in ALHE; both cases are of single lesions with hypervascularized nodular morphology, one in the dermis of the chin, which the authors describe as having the appearance of a ball of wool,5 and the other of mixed echostructure under the skin of the arm.
We report 3 histologically confirmed cases of periauricular ALHE, with ultrasound morphology that showed multiple hypervascular pseudonodular plaques in different locations than those reported previously. The description of these findings may contribute to increasing knowledge of the forms of ultrasound presentation of this disease and thus improve noninvasive diagnosis of the entity.
Clinical and Ultrasound EvaluationsThe reported cases were managed following the published recommendations of the guidelines for performing dermatologic ultrasonography and the medical ethics standards of the Declaration of Helsinki. The patients provided consent for the publication of their images and clinical data (Figs. 1 and 2, Table 1, and Video, supplementary material, Video 1).
, Clinical presentations in ALHE. Confluent erythematous, sessile papules and nodules, some of which form plaques. A), Case 1; B), Case 2; C), Dermatoscopy of Case 2; and D), Case 3.")
, Ultrasound en ALHE. A), Grayscale imaging and D), Color Doppler imaging of Case 1; B), Grayscale imaging and E), B-Flow ultrasound (General Electric Health Systems) of Case 2; C), Grayscale imaging and F), Color Doppler imaging of Case 3. Multiple diffusely hypervascular hypoechogenic dermal and superficial subcutaneous plaques with reasonably well defined edges, showing pseudonodular areas that raise and crease the epidermis, some with a polypoid exophytic appearance and with areas of epidermal, dermal and surface subcutaneous thickening. Note the vascular communication between the lesions in D-F, which was subclinical in Case 2 (B and E) and note that the superficial temporal artery (T) is near the lesion in F.")
A-F), Ultrasound en ALHE. A), Grayscale imaging and D), Color Doppler imaging of Case 1; B), Grayscale imaging and E), B-Flow ultrasound (General Electric Health Systems) of Case 2; C), Grayscale imaging and F), Color Doppler imaging of Case 3. Multiple diffusely hypervascular hypoechogenic dermal and superficial subcutaneous plaques with reasonably well defined edges, showing pseudonodular areas that raise and crease the epidermis, some with a polypoid exophytic appearance and with areas of epidermal, dermal and surface subcutaneous thickening. Note the vascular communication between the lesions in D-F, which was subclinical in Case 2 (B and E) and note that the superficial temporal artery (T) is near the lesion in F.
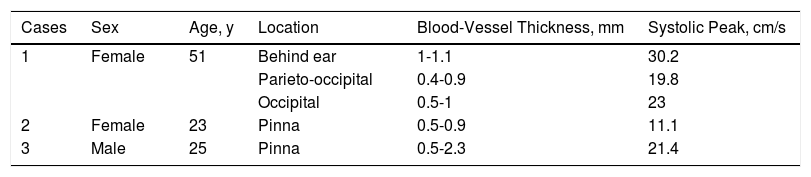
A 51-year-old previously healthy woman consulted for a lesion behind the left ear that had appeared a year earlier and had grown gradually, associated with pruritus and occasional bleeding. The physical examination revealed an erythematous multinodular tumor behind the left ear; the tumor measured 6.5×4cm and was painless to the touch.
Color Doppler ultrasound revealed 4 periauricular focal areas with a diffuse, hypervascular, hypoechogenic pseudonodular plaque-like morphology, with reasonably well defined edges and characterized by thickening and reduction of the echogenicity of the dermis, discrete undulation, and epidermal thickening and increased superficial subcutaneous echogenicity with prominent arteries of medium to low velocity. The largest plaque was located behind the left ear and measured 3.9cm on the transverse axis, 0.8cm in thickness, and 5cm on the longitudinal axis.
The second, smaller, plaque was located in the left parieto-occipital region and presented similar ultrasound characteristics. This plaque was 0.6cm wide, 0.3cm thick, and 0.8cm long. The other 2 plaques revealed similar ultrasound characteristics and were located in the left occipital region and were between 0.8 and 1.2cm wide, between 0.3 and 0.7cm thick, and between 0.8 and 1.1cm long.
No involvement of the cartilage, muscle, or underlying bone was observed.
Case 2A 23-year-old woman with no past history of interest consulted for lesions on the right pinna that had been present for 6 months and were associated with occasional otorrhagia and sensitivity of the ear canal. Physical examination revealed multiple sessile papules with a smooth surface and a maximum diameter of 0.5cm in the pinna, including the ear canal and earlobe.
Color Doppler ultrasound imaging revealed multiple hypoechogenic plaques with reasonably well defined edges and diffusely hypervascular, polypoid, exophytic, hypoechogenic pseudonodular formations located in the epidermal, dermal and superficial subcutaneous planes; the plaques were between 1.8 and 7.4mm wide, between 1.4 and 7.1mm thick, and between 2 and 5mm long and showed low-velocity arteries. In the clinical examination, these lesions appeared to be separate; however, communicating vascular pathways between the foci were observed in the dermis. No involvement of the ear cartilage was found.
Case 3A 25-year-old previously healthy man consulted for lesions in the region of the left year that had appeared 8 months earlier and were associated with occasional pruritus. Physical examination revealed multiple sessile papules and nodules with a smooth surface and a maximum diameter of 1.5cm in the left pinna.
Color Doppler ultrasound imaging revealed multiple diffusely hypervascular dermal and superficial subcutaneous hypoechogenic pseudonodular plaques with reasonably well defined edges; some of the plaques presented an exophytic appearance with dermal thickening and, to a lesser extent, epidermal and subcutaneous thickening. These formations formed a cuff surrounding the ear cartilage without compromising it and were between 3.0 and 19.3mm wide, between 4.2 and 10.6cm thick, and between 4.0 and 14.6mm long. The intralesional blood vessels showed arterial flows of medium to low velocity. The left superficial temporal artery was located 2mm ventrally to the aforementioned formations.
HistologyThe histology in these cases showed foci of epidermal hyperplasia, proliferation of capillaries and blood vessels with walls of medium thickness covered by epithelioid endothelium and with intracytoplasmic vacuoles, surrounded by a fibrous stroma with abundant lymphocytic and eosinophilic infiltrate in the dermis and epidermis compatible with ALHE (Fig. 3).
, Histology in ALHE. Hematoxylin–eosin: A), ×20; B), ×400. Dermal proliferation of capillaries and blood vessels with walls of medium thickness with epithelioid endothelium and intracytoplasmic vacuoles, abundant lymphocytic and eosinophilic infiltrate surrounded by a fibrous stroma and mild epidermal hyperplasia.")
A and B), Histology in ALHE. Hematoxylin–eosin: A), ×20; B), ×400. Dermal proliferation of capillaries and blood vessels with walls of medium thickness with epithelioid endothelium and intracytoplasmic vacuoles, abundant lymphocytic and eosinophilic infiltrate surrounded by a fibrous stroma and mild epidermal hyperplasia.
This series of cases shows a form of ultrasound presentation different from what has been reported previously and knowledge of this form of presentation may allow for improved clinical and ultrasound discrimination from other skin lesions (5,6). Moreover, the use of ultrasound imaging may help to confirm this entity in cases with multiple lesions, as in Case 1, which would avoid unnecessary biopsies and allow for noninvasive management.
Color Doppler imaging provides important anatomical data in ALHE, such as depth, involvement of deep tissue planes, such as cartilage, muscle, bone, and external orifices such as the ear canal.2,3 It also makes it possible to determine the distance to high-risk structures, such as periauricular vessels with high blood flow, such as the superficial temporal artery, which was very close to the lesions in one of the cases reported.
The finding of subclinical vascular involvement of the dermis in Case 2 is an interesting finding, as it makes it possible to understand how this entity is extended.
The differential diagnosis may include other types of angiomatous or glomangiomatous lesions, which usually present different ultrasound characteristics, often a single, more nodular, hypoechogenic, hypervascular, dermal-subcutaneous lesion (7,8).
Unlike vascular malformations,2 ALHE lesions show no tubules or internal anechogenic lacunae in the ultrasound examination and in comparison with the hypervascular variants of pilomatrixoma, ALHE lesions do not present internal hyperechogenic foci with a calcified appearance (9).
In comparison with other types of vascular tumor such as kaposiform hemangioendothelioma or angiomyxoma, the latter show less defined edges and a more heterogeneous dermal and subcutaneous echostructure.7
Another lesion that may be included in the ultrasound differential diagnosis is pyogenic granuloma, which typically presents as a single hypervascular, exophytic, hypoechogenic, polypoid lesion and does not appear as a plaque.7
Angiosarcoma usually presents in ultrasound examinations as a single hypervascular, hypoechogenic dermal and subcutaneous lesion with poorly defined, irregular or lobular edges.7
In conclusion, color Doppler ultrasound is a tool that can support the diagnosis of ALHE, and knowledge of its forms of ultrasound presentation will make it possible to improve the accuracy of the diagnosis and follow-up of the course of these cases, as well as avoiding multiple biopsies.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Wortsman X, Yagnam M, Carreño L. Morfología Ecográfica en Placa Pseudonodular Hipervascular en Hiperplasia Angiolinfoide. Actas Dermosifiliogr. 2019;110:303–307.


