

Dupilumab is a human IgG4 monoclonal antibody that targets the interleukin 4 receptor alpha (IL-4Rα), which inhibits IL-4 and IL-13. It has been approved to treat moderate-to-severe atopic dermatitis (AD), moderate-to-severe asthma, chronic rhinosinusitis with nasal polyposis, eosinophilic esophagitis, and prurigo nodularis. Regarding AD, the regimen for adults is a loading dose of 600mg, followed by 300mg every 2 weeks (Q2W).
The therapeutic optimization of biological drugs consists of down-titration in patients with a sustained good response, without loss of efficacy. This practice is rooted in psoriasis and some rheumatologic diseases to avoid unnecessary overtreatment, reduce side effects, and improve economic efficiency.1,2 Below we’ll be discussing the results of 5 studies of patients with well-controlled AD on dupilumab, in whom the dosing interval was extended beyond the above-mentioned 2-week threshold.
The first study to explore this idea was the randomized LIBERTY AD SOLO-CONTINUE clinical trial, which is a continuation of the trials that led to the approval of dupilumab for the management of AD. It studied a total of 422 patients categorized into 4 groups based on the dosing interval: Q1W/Q2W, Q4W, and Q8W. Thirty-six weeks after down-titration, no significant differences were reported in the percentage change observed in the Eczema Area and Severity Index (EASI), or in the proportion of patients with Investigator Global Assessment (IGA) 0-1 between the Q1W/Q2W and Q4W groups. Conversely, a proportion of patients with EASI-75 was lost (p=0.045), and the number of patients with, at least, a 3-point increase in the pruritus numeric rating scale (P-NRS) (p=0.02) increased. The Q8W group significantly reduced efficacy in the above-mentioned scales.3
Afterwards, a Dutch cohort of 90 patients compared the EASI of the Q2W regimen vs the Q4W and Q6W/Q8W regimens. Down-titration was gradual, first to Q3W, and then for those who maintained responses doses were further spaced out. After an, at least, 6-month follow-up, no significant EASI increases were seen in either Q4W or Q6W/Q8W. While the P-NRS remained stable in the Q4W group, it increased in the Q6W/Q8W group (p=0.01). Despite the reduced drug levels, the severity biomarkers PARC/CCL18 and TARC/CCL17 remained low.1
A French series of 88 patients identified 3 predictors of sustained response after dose reduction: spacing due to good sustained response rather than side effects (p=0.034), older age (p=0.006), and lower monthly dose of topical corticosteroids (0.016). Data from the reviewed studies are summarized in Table 1.4
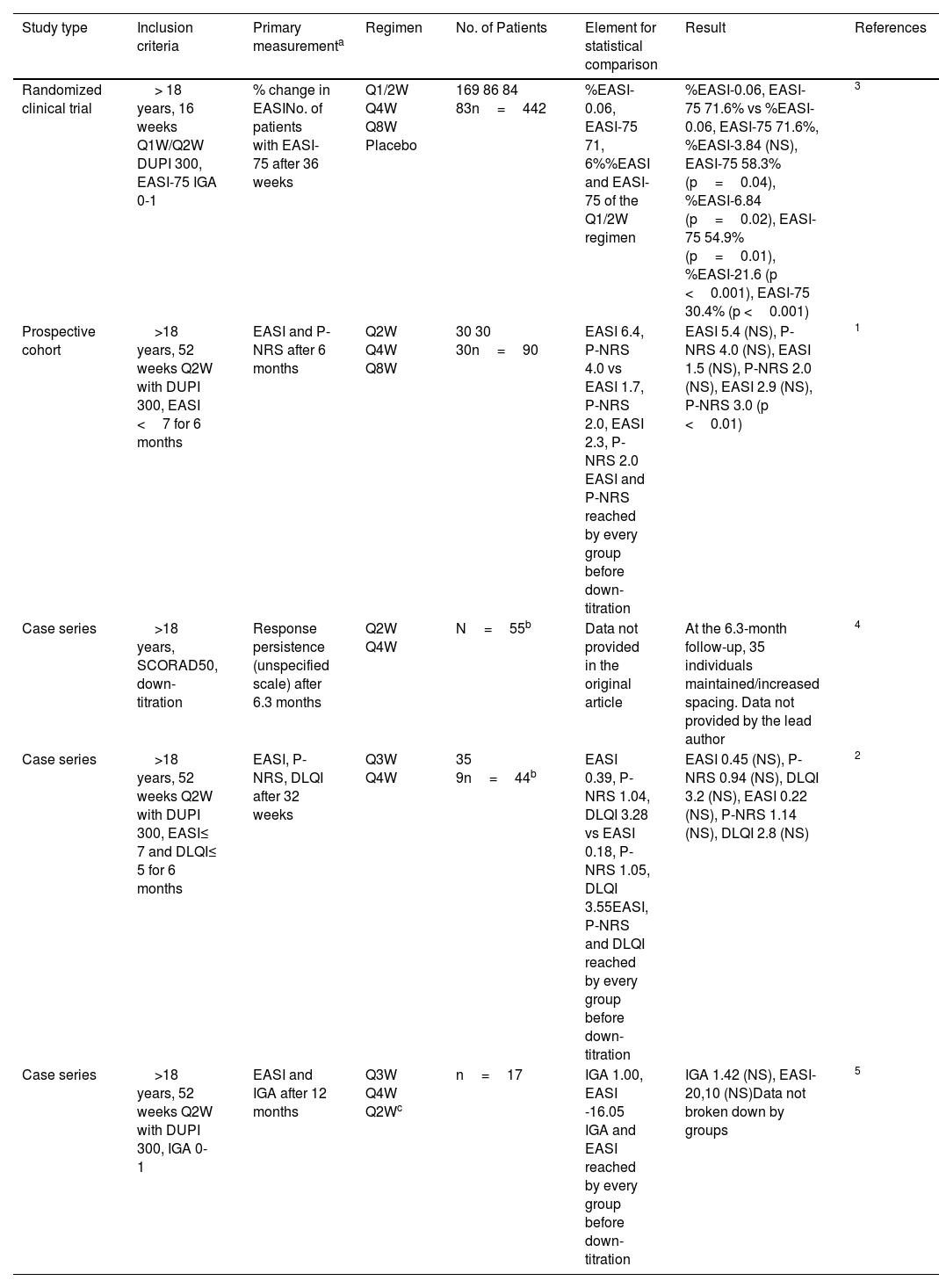
Studies in which the dupilumab dose was spaced out due to sustained good response.
| Study type | Inclusion criteria | Primary measurementa | Regimen | No. of Patients | Element for statistical comparison | Result | References |
|---|---|---|---|---|---|---|---|
| Randomized clinical trial | > 18 years, 16 weeks Q1W/Q2W DUPI 300, EASI-75 IGA 0-1 | % change in EASINo. of patients with EASI-75 after 36 weeks | Q1/2W Q4W Q8W Placebo | 169 86 84 83n=442 | %EASI-0.06, EASI-75 71, 6%%EASI and EASI-75 of the Q1/2W regimen | %EASI-0.06, EASI-75 71.6% vs %EASI-0.06, EASI-75 71.6%, %EASI-3.84 (NS), EASI-75 58.3% (p=0.04), %EASI-6.84 (p=0.02), EASI-75 54.9% (p=0.01), %EASI-21.6 (p <0.001), EASI-75 30.4% (p <0.001) | 3 |
| Prospective cohort | >18 years, 52 weeks Q2W with DUPI 300, EASI <7 for 6 months | EASI and P-NRS after 6 months | Q2W Q4W Q8W | 30 30 30n=90 | EASI 6.4, P-NRS 4.0 vs EASI 1.7, P-NRS 2.0, EASI 2.3, P-NRS 2.0 EASI and P-NRS reached by every group before down-titration | EASI 5.4 (NS), P-NRS 4.0 (NS), EASI 1.5 (NS), P-NRS 2.0 (NS), EASI 2.9 (NS), P-NRS 3.0 (p <0.01) | 1 |
| Case series | >18 years, SCORAD50, down-titration | Response persistence (unspecified scale) after 6.3 months | Q2W Q4W | N=55b | Data not provided in the original article | At the 6.3-month follow-up, 35 individuals maintained/increased spacing. Data not provided by the lead author | 4 |
| Case series | >18 years, 52 weeks Q2W with DUPI 300, EASI≤ 7 and DLQI≤ 5 for 6 months | EASI, P-NRS, DLQI after 32 weeks | Q3W Q4W | 35 9n=44b | EASI 0.39, P-NRS 1.04, DLQI 3.28 vs EASI 0.18, P-NRS 1.05, DLQI 3.55EASI, P-NRS and DLQI reached by every group before down-titration | EASI 0.45 (NS), P-NRS 0.94 (NS), DLQI 3.2 (NS), EASI 0.22 (NS), P-NRS 1.14 (NS), DLQI 2.8 (NS) | 2 |
| Case series | >18 years, 52 weeks Q2W with DUPI 300, IGA 0-1 | EASI and IGA after 12 months | Q3W Q4W Q2Wc | n=17 | IGA 1.00, EASI -16.05 IGA and EASI reached by every group before down-titration | IGA 1.42 (NS), EASI-20,10 (NS)Data not broken down by groups | 5 |
All significant changes were due to loss of efficacy in some scale.
When multiple measurements were available, the most recent one was used, except in 4 where only the described data was available.
In conclusion, various authors propose a consensual and gradual down-titration of dupilumab in well-controlled patients. It has been hypothesized that the sustained response is due to the selection of super responders, in whom a lower drug level saturates the pharmacological target.1,2,4,5 Conducting controlled studies aims to avoid iatrogenesis and promote efficiency with the advent of new drugs.



