


The presence of skin lesions is a common finding in hospitalized patients. In fact, in some cases, the skin can be an expression of systemic diseases that can jeopardize the patients’ lives.1 The swift detection and identification of these changes can have a tremendous impact on the length of stay and the patient's outcomes.2–4 Inaccurate diagnoses may lead to unnecessary tests and treatments, increase iatrogeny, impact the medical outcomes, and be detrimental to these patients’ quality of life.5,6 The objective of this study was to provide a description of the dermatologic consultations of a tertiary referral hospital. This report intends to generate future hypotheses to improve the management of these patients.
This was a retrospective descriptive study conducted to gather all consecutive hospital dermatologic consultations reported at Hospital Universitario y Politécnico La Fe, Valencia, Spain from January 1, 2022 to December 31, 2022. All consultations were evaluated by, at least, 2 dermatologists. Patients were seen the same day, or the day after the consultation. Data mining and initial manuscript drafting were performed by the first 3 authors (MMP, FNB, and DMT), while the final manuscript was completed by the fourth author (RBE). Statistical analysis was conducted using IBM® SPSS® statistical software package, version 27.0.
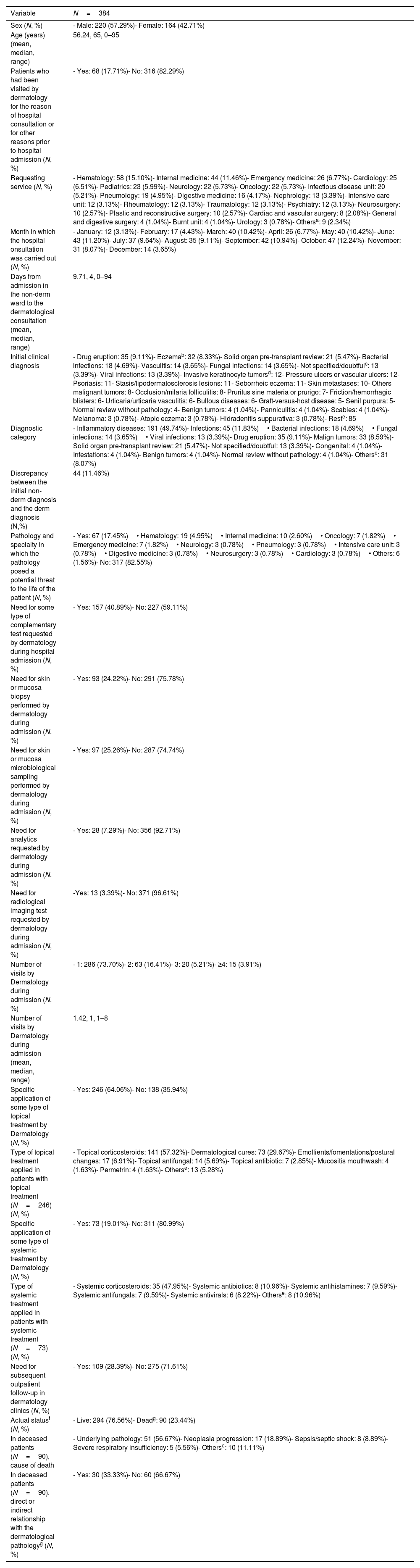
The study results are shown in Table 1. A total of 384 consultations were collected. Of these, 57% and 42% were male and female patients, respectively, with a mean age of 56 years. The hospital units that most commonly requested dermatologic consultations were hematology (15%), and internal medicine (11%). The median time from admission to consultation was 4 days. Regarding the reasons for consultation, the most common dermatologic diagnostic category was inflammatory diseases (almost 50% of the sample), although the single most common reason for consultation was drug eruptions (9%). Notably, almost 9% of all consultations were associated with malignant tumors, and up to 17% of all diagnoses presented with a level of severity that could jeopardize the patient's life. All additional tests were performed or requested by the dermatology unit during admission. Additionally, microbiological samples were obtained from 25% of the patients, biopsies from 24%, blood tests were performed in 7%, and radiological imaging were obtained in 3% of the patients. Most of them (74%) received only 1 visit during admission. Nearly 64% of the patients received some form of topical treatment, being topical corticosteroids and wound dressings the most common of all. On the other hand, 19% received systemic treatment, and 23% of the patients died within the months following admission, being their underlying condition the most common cause of death. Finally, one-third of the patients (33%) died directly or indirectly due to the dermatological condition that triggered the consultation in the first place.
Results of the analysis carried out.
| Variable | N=384 |
|---|---|
| Sex (N, %) | - Male: 220 (57.29%)- Female: 164 (42.71%) |
| Age (years) (mean, median, range) | 56.24, 65, 0–95 |
| Patients who had been visited by dermatology for the reason of hospital consultation or for other reasons prior to hospital admission (N, %) | - Yes: 68 (17.71%)- No: 316 (82.29%) |
| Requesting service (N, %) | - Hematology: 58 (15.10%)- Internal medicine: 44 (11.46%)- Emergency medicine: 26 (6.77%)- Cardiology: 25 (6.51%)- Pediatrics: 23 (5.99%)- Neurology: 22 (5.73%)- Oncology: 22 (5.73%)- Infectious disease unit: 20 (5.21%)- Pneumology: 19 (4.95%)- Digestive medicine: 16 (4.17%)- Nephrology: 13 (3.39%)- Intensive care unit: 12 (3.13%)- Rheumatology: 12 (3.13%)- Traumatology: 12 (3.13%)- Psychiatry: 12 (3.13%)- Neurosurgery: 10 (2.57%)- Plastic and reconstructive surgery: 10 (2.57%)- Cardiac and vascular surgery: 8 (2.08%)- General and digestive surgery: 4 (1.04%)- Burnt unit: 4 (1.04%)- Urology: 3 (0.78%)- Othersa: 9 (2.34%) |
| Month in which the hospital onsultation was carried out (N, %) | - January: 12 (3.13%)- February: 17 (4.43%)- March: 40 (10.42%)- April: 26 (6.77%)- May: 40 (10.42%)- June: 43 (11.20%)- July: 37 (9.64%)- August: 35 (9.11%)- September: 42 (10.94%)- October: 47 (12.24%)- November: 31 (8.07%)- December: 14 (3.65%) |
| Days from admission in the non-derm ward to the dermatological consultation (mean, median, range) | 9.71, 4, 0–94 |
| Initial clinical diagnosis | - Drug eruption: 35 (9.11%)- Eczemab: 32 (8.33%)- Solid organ pre-transplant review: 21 (5.47%)- Bacterial infections: 18 (4.69%)- Vasculitis: 14 (3.65%)- Fungal infections: 14 (3.65%)- Not specified/doubtfulc: 13 (3.39%)- Viral infections: 13 (3.39%)- Invasive keratinocyte tumorsd: 12- Pressure ulcers or vascular ulcers: 12- Psoriasis: 11- Stasis/lipodermatosclerosis lesions: 11- Seborrheic eczema: 11- Skin metastases: 10- Others malignant tumors: 8- Occlusion/milaria folliculitis: 8- Pruritus sine materia or prurigo: 7- Friction/hemorrhagic blisters: 6- Urticaria/urticaria vasculitis: 6- Bullous diseases: 6- Graft-versus-host disease: 5- Senil purpura: 5- Normal review without pathology: 4- Benign tumors: 4 (1.04%)- Panniculitis: 4 (1.04%)- Scabies: 4 (1.04%)- Melanoma: 3 (0.78%)- Atopic eczema: 3 (0.78%)- Hidradenitis suppurativa: 3 (0.78%)- Reste: 85 |
| Diagnostic category | - Inflammatory diseases: 191 (49.74%)- Infections: 45 (11.83%)• Bacterial infections: 18 (4.69%)• Fungal infections: 14 (3.65%)• Viral infections: 13 (3.39%)- Drug eruption: 35 (9.11%)- Malign tumors: 33 (8.59%)- Solid organ pre-transplant review: 21 (5.47%)- Not specified/doubtful: 13 (3.39%)- Congenital: 4 (1.04%)- Infestations: 4 (1.04%)- Benign tumors: 4 (1.04%)- Normal review without pathology: 4 (1.04%)- Otherse: 31 (8.07%) |
| Discrepancy between the initial non-derm diagnosis and the derm diagnosis (N,%) | 44 (11.46%) |
| Pathology and specialty in which the pathology posed a potential threat to the life of the patient (N, %) | - Yes: 67 (17.45%)• Hematology: 19 (4.95%)• Internal medicine: 10 (2.60%)• Oncology: 7 (1.82%)• Emergency medicine: 7 (1.82%)• Neurology: 3 (0.78%)• Pneumology: 3 (0.78%)• Intensive care unit: 3 (0.78%)• Digestive medicine: 3 (0.78%)• Neurosurgery: 3 (0.78%)• Cardiology: 3 (0.78%)• Others: 6 (1.56%)- No: 317 (82.55%) |
| Need for some type of complementary test requested by dermatology during hospital admission (N, %) | - Yes: 157 (40.89%)- No: 227 (59.11%) |
| Need for skin or mucosa biopsy performed by dermatology during admission (N, %) | - Yes: 93 (24.22%)- No: 291 (75.78%) |
| Need for skin or mucosa microbiological sampling performed by dermatology during admission (N, %) | - Yes: 97 (25.26%)- No: 287 (74.74%) |
| Need for analytics requested by dermatology during admission (N, %) | - Yes: 28 (7.29%)- No: 356 (92.71%) |
| Need for radiological imaging test requested by dermatology during admission (N, %) | -Yes: 13 (3.39%)- No: 371 (96.61%) |
| Number of visits by Dermatology during admission (N, %) | - 1: 286 (73.70%)- 2: 63 (16.41%)- 3: 20 (5.21%)- ≥4: 15 (3.91%) |
| Number of visits by Dermatology during admission (mean, median, range) | 1.42, 1, 1–8 |
| Specific application of some type of topical treatment by Dermatology (N, %) | - Yes: 246 (64.06%)- No: 138 (35.94%) |
| Type of topical treatment applied in patients with topical treatment (N=246) (N, %) | - Topical corticosteroids: 141 (57.32%)- Dermatological cures: 73 (29.67%)- Emollients/fomentations/postural changes: 17 (6.91%)- Topical antifungal: 14 (5.69%)- Topical antibiotic: 7 (2.85%)- Mucositis mouthwash: 4 (1.63%)- Permetrin: 4 (1.63%)- Otherse: 13 (5.28%) |
| Specific application of some type of systemic treatment by Dermatology (N, %) | - Yes: 73 (19.01%)- No: 311 (80.99%) |
| Type of systemic treatment applied in patients with systemic treatment (N=73) (N, %) | - Systemic corticosteroids: 35 (47.95%)- Systemic antibiotics: 8 (10.96%)- Systemic antihistamines: 7 (9.59%)- Systemic antifungals: 7 (9.59%)- Systemic antivirals: 6 (8.22%)- Otherse: 8 (10.96%) |
| Need for subsequent outpatient follow-up in dermatology clinics (N, %) | - Yes: 109 (28.39%)- No: 275 (71.61%) |
| Actual statusf (N, %) | - Live: 294 (76.56%)- Deadg: 90 (23.44%) |
| In deceased patients (N=90), cause of death | - Underlying pathology: 51 (56.67%)- Neoplasia progression: 17 (18.89%)- Sepsis/septic shock: 8 (8.89%)- Severe respiratory insufficiency: 5 (5.56%)- Otherse: 10 (11.11%) |
| In deceased patients (N=90), direct or indirect relationship with the dermatological pathologyg (N, %) | - Yes: 30 (33.33%)- No: 60 (66.67%) |
Early recognition of skin lesions can have an impact on the patients’ prognosis. This becomes even more evident in hospitalized patients, who often present with more severe conditions than outpatient individuals.1,7 As far as we know, ours is one of the longest series ever reported of dermatologic consultations.
Most patients were admitted to the hematology and internal medicine units, and the most common reasons for consultation were inflammatory conditions. This finding is consistent with what other series have reported on this regard.2,3,7,8 Unlike other series, it is striking that the single most common diagnosis was drug eruptions. While most of these cases were mild, very severe cases of toxicoderma were also reported, such as up to 4 cases of toxic epidermal necrolysis (Fig. 1). An increased incidence of these types of lesions is expected. This is possibly due to polypharmacy, the development of new targets and therapeutic agents, and the patients’ overall higher life expectancy.9 Despite most consultations being associated with mild conditions, almost 20% of them could potentially threaten the patients’ lives. These data emphasize the importance of hospital dermatology units. Also, we should mention the wide range of additional tests a dermatologist can request or perform, including biopsies, microbiological cultures, blood, or urine tests, and imaging modalities. In our series, almost a quarter of the patients underwent additional tests, a slightly higher rate than that reported in the current scientific medical literature available.1–3,5,8 This is likely due to the complexity of the patients treated in our center.
, and upper back region (panel B). In the following days. The patient")
Example of a 53-year-old woman who presented to the dermatologic consultation with pembrolizumab-related toxic epidermal necrolysis against metastatic lung cancer. Exanthema was predominant over the face, neckline (panel A), and upper back region (panel B). In the following days. The patient's lesions progressed until they covered 60% of the body surface area.
Our study has some limitations. Firstly, biases derived from its retrospective nature. We did not analyze the agreement between dermatologic and non-dermatologic diagnoses either. On the other hand, a comprehensive test of the diseases on a monthly basis was not conducted, for example if viral exanthemas are more common in winter or arthropod bites in the summertime. Finally, the hospital where the tests were conducted assists a large volume of hematological and oncological patients. This may bias the results as more cases of drug eruptions or malignant neoplasms may have been reported.
In conclusion, this case report underscores the importance of dermatology in the management of patients admitted to non-dermatology wards.
Conflict of interestThe authors declare that they have no conflict of interest.


