

Cutaneous squamous cell carcinoma (cSCC) is a common cancer,1 Incidence of cSCC varies across countries. In the United States was 497 in men and 296 in women per 100,000 inhabitants/year, whereas in Germany was 54 and 26, respectively, and in Spain was 38 new cases/100,000 inhabitants/year.2,3
In Uruguay, the latest data published are from the 2010–2014 period and reported an incidence of cSCC in women of 5.11 cases per 100,000 inhabitants and in men of 13.10 cases per 100,000 inhabitants.4
Hospital de Clínicas “Dr. Manuel Quintela”, located in Montevideo, Uruguay, is the only public center that has Mohs Micrographic Surgery (MMS) in the country.
This work aims to determine the epidemiological and clinical characteristics of high risk cSCCs that underwent MMS over a period of 5 years.
A transversal, retrospective, descriptive study was conducted, which included all the cSCCs operated by MMS in the surgery unit of our medical service between November 2013 and November 2018. Dermatologist-referred patients or with histopathological diagnosis of cSCC and indication of CMM were included.
The epidemiological variables of sex, age at the time of diagnosis, department of origin of the patient and clinical variables, such as phototype, location of the lesions, their correlation with the histological type and whether it was a primary tumor versus a relapse, were studied (Fig. 1).

Data collection was obtained from the review of surgical records.
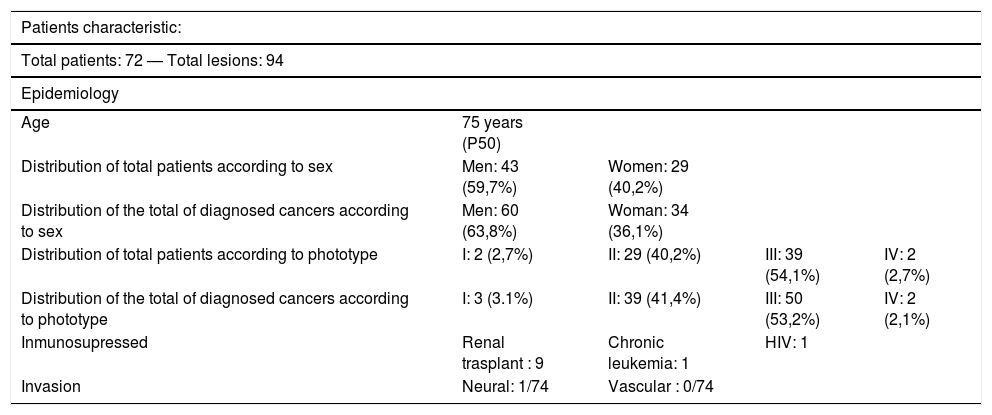
72 patients were included, with epidemiological characteristics described in Table 1.
Epidemiology and characteristics of the studied patients.
| Patients characteristic: | ||||
|---|---|---|---|---|
| Total patients: 72 — Total lesions: 94 | ||||
| Epidemiology | ||||
| Age | 75 years (P50) | |||
| Distribution of total patients according to sex | Men: 43 (59,7%) | Women: 29 (40,2%) | ||
| Distribution of the total of diagnosed cancers according to sex | Men: 60 (63,8%) | Woman: 34 (36,1%) | ||
| Distribution of total patients according to phototype | I: 2 (2,7%) | II: 29 (40,2%) | III: 39 (54,1%) | IV: 2 (2,7%) |
| Distribution of the total of diagnosed cancers according to phototype | I: 3 (3.1%) | II: 39 (41,4%) | III: 50 (53,2%) | IV: 2 (2,1%) |
| Inmunosupressed | Renal trasplant : 9 | Chronic leukemia: 1 | HIV: 1 | |
| Invasion | Neural: 1/74 | Vascular : 0/74 | ||
In Uruguay, in relation to the epidemiological characteristics evaluated, genre and age range of patients are consistent with the reported in the literature,1,5 emphasize that the majority were male patients, at advanced ages, in individuals with low phototypes, located in photoexposed sectors and some had more than one cancer at the same time. We observed a clear preponderance of number of patients and cancer in low phototypes, II and III, according to the predominant ethnic groups in Uruguay (Table 2).6,7
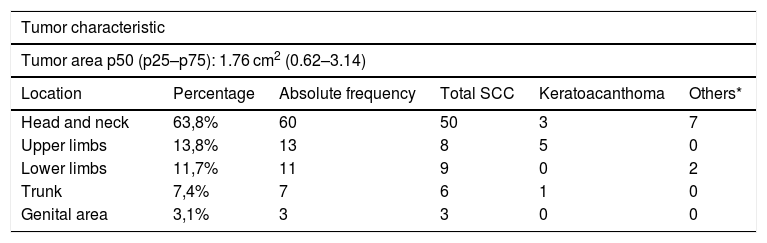
Size, location and recurrence of the tumors.
| Tumor characteristic | |||||
|---|---|---|---|---|---|
| Tumor area p50 (p25–p75): 1.76 cm2 (0.62–3.14) | |||||
| Location | Percentage | Absolute frequency | Total SCC | Keratoacanthoma | Others* |
| Head and neck | 63,8% | 60 | 50 | 3 | 7 |
| Upper limbs | 13,8% | 13 | 8 | 5 | 0 |
| Lower limbs | 11,7% | 11 | 9 | 0 | 2 |
| Trunk | 7,4% | 7 | 6 | 1 | 0 |
| Genital area | 3,1% | 3 | 3 | 0 | 0 |
| Previous treatment in recurrences patients | ||
|---|---|---|
| Type of procedure | Number of recurrences n = 14 | Recurrence onset time in months, median (RIC) |
| Conventional surgery | 5 | 7,5 (3–12) |
| Mohs surgery | 2 | 15,5 (13,75–17,25) |
| Other treatment** | 7 | 36 (12–48) |
In our patients, the topography most affected by squamous cell carcinoma was the head and neck, perhaps due that are the most affected common photoexposed areas and to the lack of photoprotection/photoeducation in the population. In a prospective study of 1263 patients, reported that 95.6% of the SCCs were located in the head and neck, the most frequently affected areas being ears, cheeks and nose.5
Well-differentiated cSCC followed by the SCC in situ were the most frequent histological type, this is probably due to the fact that in our Hospital we have a high index of suspicion of malignant lesions, we can detect the tumor at an early stage, thus avoiding the possibility of unfavorable progression of the lesion. Compared with a regional study conducted in Brazil where 1437 SCC were studied, of which 77% corresponded to a well differentiated SCC.8
In our patients, 14 patients had been treated previously by any modality. Two of them was treated by Mohs surgery. Lee et al. reported a recurrence of 3% in MMS vs 8% of standard excision.9
According to the Comisión Honoraria de Lucha contra el Cáncer (CHLCC), between 2007 and 2011, were distributed approximately 50% in Montevideo and the other 50% in the provinces.4 In regard to the variation of solar irradiation, the territorial variation turns out to be much less than the seasonal, due to the relative geographical uniformity of our territory. The coastal sites in the south (Rocha, Maldonado, Montevideo) have the lowest average irradiation, while the highest values appear in the north (Artigas, Rivera, Salto, Paysandú).10 According to our work, 28/72 would be patients from Montevideo. The distribution of the origin of patients operated by MSS in Uruguay is curious, since the largest number of cases are concentrated in the capital and its periphery. This is probably due to the greater amount of population located in this sector, the possibility of patient transfer, the proximity to the center, the number of professionals and the provision of the technique in Montevideo.
However, it is striking that in 5 years, there are areas with no reports of patients operated by MSS in our center, possibly corresponding to 3 alternatives: the first one, that they had a rapid transfer and the tumors were low risk; the second, that they were operated in another center; or the third, that there is a subdiagnosis.
Please cite this article as: Correa Sanino JFE, Cabanelas Ferrando L, Magliano Lopez JC, Bazzano Perez CI, Características clínico-epidemiológicas del carcinoma de células escamosas operado mediante cirugía micrográfica de Mohs en Uruguay, ACTAS Dermo-Sifiliográficas, 2021, https://doi.org/10.1016/j.ad.2020.07.005


