





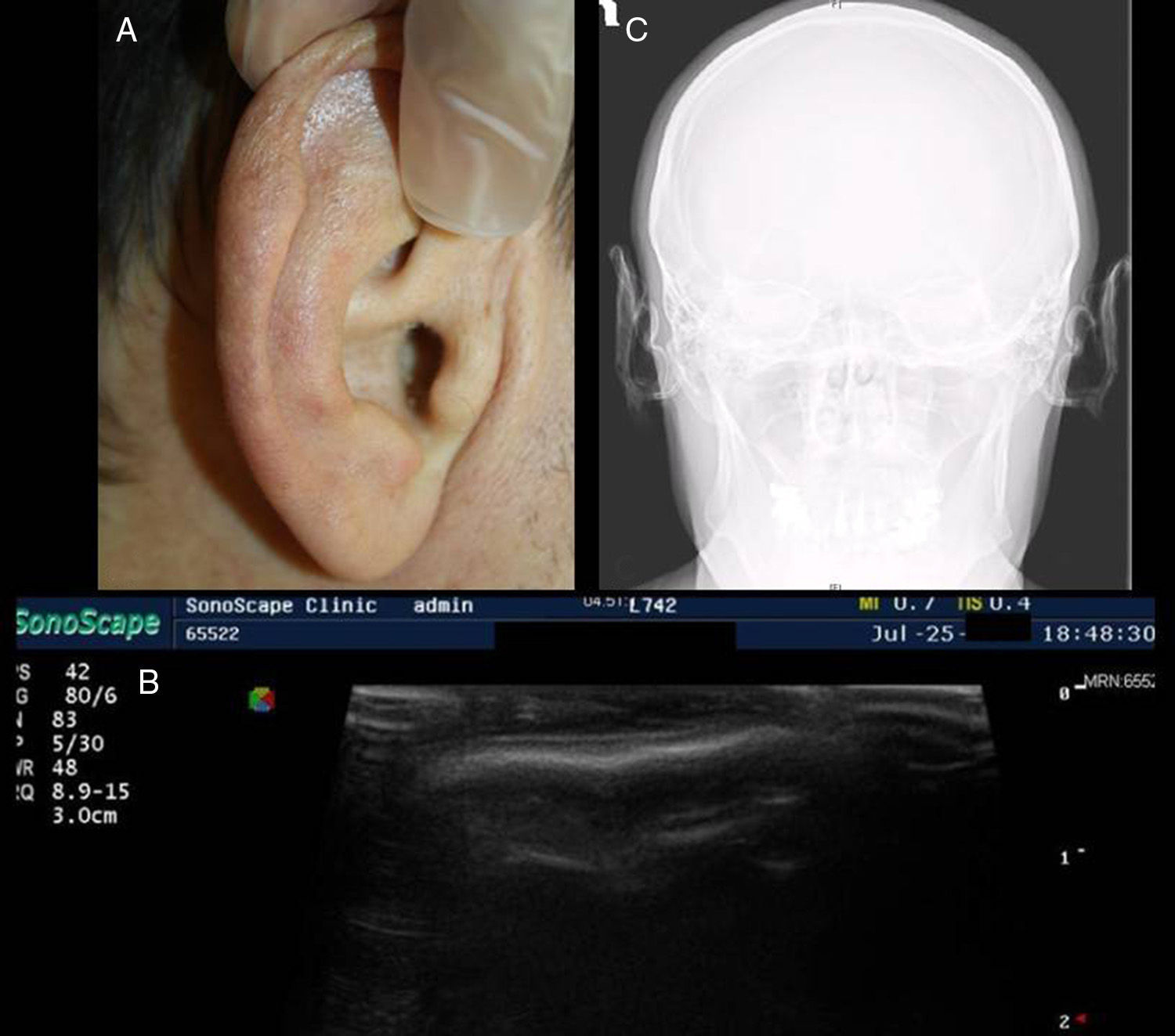
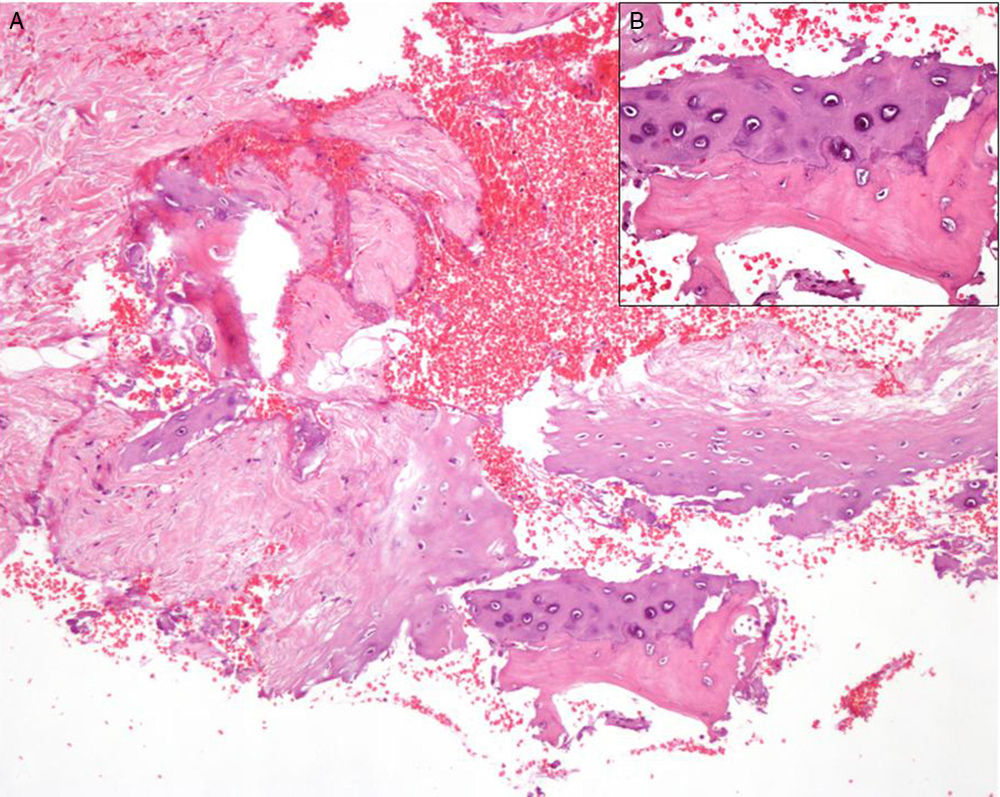
We present the case of a 45-year-old man who was admitted for hyponatremia of unknown etiology. He was referred to Dermatology by Internal Medicine for evaluation of an induration of the auricles of the ears. On examination, the ears were of normal appearance, with no visible changes in the skin. Palpation revealed diffuse rigidity of the cartilaginous part of the auricle bilaterally, with no changes in the ear lobes (Fig. 1A). The patient stated that the changes had started 2 years earlier and had been progressive and asymptomatic. Skin ultrasound revealed a hypoechoic area corresponding to the normal auricular cartilage, superficial to which there was a linear hyperechoic image suggestive of transformation of the cartilage by mineralization (Fig. 1B). On cranial x-ray, the auricles of the ear showed a diffuse and homogeneous increase in density, similar to that of bone (Fig. 1C). Histopathology of the skin and of the auricular cartilage showed no significant changes in the epidermis or dermis, but there were fragments of elastic cartilage with foci of ossification and the formation of mature bone trabeculae (Fig. 2, A andB).
In the blood tests, the basal cortisol levels were almost undetectable (<0.4μg/dL; normal range, 4.3-22.4μg/dL), with corticotropin levels in the lower range of normal (9.5pg/mL; normal range, 8-46pg/mL) and an inadequate cortisol response in the corticotropin stimulation test (cortisol, 1.11μg/dL). The prolactin level was slightly elevated (47.8ng/mL; normal range, 2.6-13.1ng/mL). Studies of calcium metabolism, other hormonal markers, autoimmunity, and serology for infectious diseases were normal or negative. No changes were observed on abdominal ultrasound, cerebral computed tomography, or magnetic resonance imaging of the hypophysis. A diagnosis was made of bilateral ossification of the auricles secondary to central adrenal insufficiency of unknown origin.
Auricular ossification is a very rare cause of petrified auricles, a condition first described by Bochdalek1 in 1866 and which has now been reported in the literature in more than 160 cases. The most common cause of petrified auricles is auricular calcification, which is associated with numerous diseases and, as occurs with calcinosis cutis, it can be metastatic, dystrophic, or idiopathic. In auricular ossification, ectopic bone formation is a response to the release of bone morphogenetic protein by damaged tissue.1 New bone forms over tissues that do not normally ossify; this occurs by the deposition of calcium and phosphorus salts in a proteinaceous matrix of hydroxyapatite crystals. Severe or recurrent hypothermia is the most common cause of auricular ossification,2,3 though the condition has also be described secondary to trauma and local inflammatory conditions. The systemic disease most commonly associated with auricular ossification is adrenal insufficiency, although the pathophysiological mechanism is unclear.4–6 It has been suggested that an acute or chronic fall in cortisol levels may induce a reactive hypercalcemia that could lead to calcium deposition in tissues, such as acral tissues, made susceptible by a poor peripheral circulation; however, this hypothesis is still in doubt because many patients have no detectable hypercalcemia.
The disorder mainly affects men. On examination there is a typically asymptomatic, partial or complete induration of the auricle of the ear with sparing of the ear lobe; there are no visible alterations of the skin. Some patients present pain on pressure and, in a few cases, pressure ulcers may develop.4 In addition, alterations of the external auditory canal can lead to secondary otalgia and hearing impairment. The rigidity is most commonly bilateral and progressive. The clinical findings enable a provisional diagnosis to be established and this will be supported by the radiologic findings; however, the definitive diagnosis of auricular ossification is established on histology, which reveals replacement of the auricular cartilage by true lamellar bone, with the presence of bone trabeculae and osteocytes.7,8 The etiologic diagnosis is based on a full medical history including possible inflammatory disorders and trauma. Only when no local cause can be identified should laboratory screening studies be performed to exclude underlying metabolic or endocrinologic diseases. There is no specific treatment for this condition and its course is irreversible.7,8 In patients who report pain, some authors favor treatment by surgical reduction of the affected auricle.8,9
Twenty cases of histologically documented auricular ossification have been reported to date in the literature (Table 1). Of these, 4 cases were associated with systemic diseases: 3 with primary adrenal insufficiency4,5 and 1 with adrenal insufficiency secondary to postpartum hypopituitarism.6 We have reported the second case of auricular ossification associated with secondary adrenal insufficiency. It is important for dermatologists to be able to recognize this pathological entity as it may sometimes be the only manifestation of an underlying metabolic or endocrinologic disease that can often be subclinical.
Data From 21 Documented Cases of Auricular Ossification.
| Author | Sex/Age, y | Site | Cause |
|---|---|---|---|
| Present case | M/46 | Bilateral | Secondary adrenal insufficiency |
| Kim et al.10(2011) | M/53 | Unilateral (L) | Trauma |
| Machado et al.6(2009) | F/57 | Bilateral | Postpartum hypopituitarism |
| Mastronikolis et al.4(2009) | M/73 | Bilateral | Primary adrenal insufficiency (AD) |
| Carfrae-Foyt (2008) | M/49 | Unilateral (L) | Unknown |
| Sterneberg-Vos et al. (2007) | M/70 | Unilateral (R) | Hypothermia |
| González-Sixto et al.3(2006) | M/65 | Bilateral | Hypothermia |
| Manni et al.8(2005) | F/63 | Bilateral | Unknown |
| High et al. (2004) | M/60 | Bilateral | Unknown |
| Stites et al. (2003) | M/65 | Unilateral (L) | Frostbite |
| Yeatman and Varigos (1998)7 | M/66 | Unilateral (R) | Hypothermia |
| Lautenschlager et al. (1994) | M/66 | Bilateral | Hypothermia |
| Cohen et al. (1991)5 | M/46 | Bilateral | Primary adrenal insufficiency (AD) |
| Lari et al. (1989)9 | M/17 | Bilateral | Trauma |
| Cohen et al. (1989) | M/70 | Bilateral | Primary adrenal insufficiency (AD) |
| Di Bartolomeo (1985)2 | M/77 | Bilateral | Frostbite |
| M/72 | Bilateral | Frostbite | |
| Lister (1969) | M/58 | Bilateral | Unknown |
| Gordon (1964) | F/34 | Bilateral | Perichondritis |
| Scherrer (1932) | F/53 | Bilateral | Unknown |
| Knapp (1890) | M/24 | Unilateral | Perichondritis |
Abbreviations: AD, Addison disease; F, female; L, left; M: male, R, right.
Please cite this article as: Calderón-Komáromy A, Córdoba S, Tardío JC, Borbujo J. Osificación bilateral del cartílago auricular. Actas Dermosifiliogr. 2015;106:433–435.


