

Countless sex education programs have been implemented worldwide in recent decades, but epidemiological data show no improvement in rates of sexually transmitted infections or unintended pregnancies.
ObjectiveTo summarize the evidence from higher-quality systematic reviews on the efficacy of behavioral interventions for the prevention of sexually transmitted infections and unintended pregnancies.
MethodsWe conducted an overview of reviews by selecting systematic reviews that met minimum quality criteria in terms of the design of the studies reviewed. We compared the results obtained when the effects of interventions were assessed on the basis of objective criteria (biological data) to those obtained when outcomes were assessed on the basis of subjective criteria (self-reports). The results of Cochrane and non-Cochrane reviews were also compared.
ResultsWe identified 55 systematic reviews. No overall effect on the sexual behavior of program participants was observed in 72.5% of the reviews that used objective criteria and in 48.1% of the reviews based on subjective criteria. In the Cochrane reviews, no evidence of an overall effect was observed in 86% of reviews based on objective variables and in 70.5% of those based on subjective variables.
ConclusionsThere is no evidence that behavioral interventions modify rates of sexually transmitted infections (including human immunodeficiency virus infections) or unintended pregnancies, particularly when effects are assessed using objective, biological data. Primary prevention strategies for sexually transmitted infections and unintended pregnancies need to be re-evaluated.
En los últimos decenios se han desarrollado muchos programas de educación sexual en todo el mundo. Los datos epidemiológicos no indican una mejoría en las tasas de infecciones de transmisión sexual y embarazo no deseado.
ObjetivosSintetizar la evidencia de las revisiones sistemáticas de mayor calidad sobre la eficacia de las intervenciones conductuales para la prevención de infecciones de transmisión sexual y embarazo no deseado.
MétodosSe diseñó una «revisión de revisiones» seleccionando revisiones sistemáticas que cumpliesen unos criterios de calidad mínimos (en función del diseño de los estudios que incluyen). Se compararon los resultados obtenidos al evaluar los efectos de las intervenciones mediante criterios objetivos (datos biológicos) con los conseguidos al evaluarlos mediante criterios subjetivos (autoinforme), así como en función de si se trataba o no de una revisión Cochrane.
ResultadosSe identificaron 55 revisiones sistemáticas. En el 72,5% no se observó efecto global de las intervenciones en la conducta sexual de los participantes, evaluada mediante variables objetivas. Cuando se evaluaban las intervenciones mediante resultados subjetivos, no se detectó efecto global en el 48,1% de las revisiones. El 86,6% de las revisiones Cochrane no observaron efecto al usar variables objetivas, y el 70,5% no lo detectaron mediante variables subjetivas.
ConclusiónNo hay evidencia de que las intervenciones conductuales modifiquen las tasas de infección de transmisión sexual (incluyendo el virus de la inmunodeficiencia humana) ni de embarazo no deseado, sobre todo cuando se evalúan mediante resultados biológicos objetivos. Es importante reevaluar las estrategias de prevención primaria en infecciones de transmisión sexual y embarazo no deseado.
Sexually transmitted infections (STIs) and unintended pregnancies are significant problems that are directly related to sexual behaviors.
The World Health Organization estimates that the incidence of STIs increased 40% between 1995 and 2012.1
Epidemiologic data and observational studies suggest that there has also been no improvement in the rates of unintended pregnancies. It was estimated that 49% of all pregnancies in the United States in 2006 were unintended and that the prevalence of such pregnancies rose to 80% in the age bracket of 19 years and under.2,3 One observational study covering 20 years of data for the US showed that the overall unintended birth rates were not falling.4
We note that the deterioration in these statistics has been accompanied by ever more widespread implementation of primary preventive measures, especially behavioral interventions.
In addition, spending on such programs in countries with low-to-middle income levels per capita, with the sole purpose of preventing human immunodeficiency virus (HIV) infections, was estimated to reach US $23000 million in 2015.5
Given this scenario, some health authorities have come to realize that so-called sexual education has not had, nor will it ever have, the desired results, and so they now recommend long-acting contraceptive methods such as intrauterine devices.6 The situation is the same for STIs: more and more institutions recommend so-called biomedical prophylaxis (preexposure antibiotics and/or antiretroviral drugs), suggesting loss of faith in the efficacy of behavioral interventions alone.7
The approach of evidence-based medicine should assist with decision-making by providing an assessment of available evidence for the true efficacy of these preventive strategies,8 and taking into consideration the special problems of trials to determine the impact of behavioral interventions on STIs and unintended pregnancies:
- -
Double-blind trials are not undertaken because of the nature of the clinical context.
- -
The widespread use of subjective outcomes to assess the effect of behavioral interventions is a well recognized source of bias. In one study, 16% of participants who initially reported having had sexual relations at baseline stated 6 months later that they had never had any sexual intercourse.9 For this reason study designers increasingly insist on the inclusion of biological markers of sexual activity (tests to confirm STIs, pregnancy, and semen exposure, notably detection of plasma prostate antigen or Y chromosome DNA.10
- -
Some trials report irrational contradictions: it is common to see results like those described by Lu et al.,11 in which condom use and knowledge of HIV increased significantly in intervention groups while the number of sexual partners decreased, yet the groups’ prevalences of HIV infection and syphilis did not fall or may have even risen.
These difficulties have enormous social and economic impact. This overview of systematic reviews provides a clinically relevant and coherent description of all the information available on the efficacy of interventions targeting sexual behavior. The overview is intended to aid physicians, policy-makers, educators, and patients.
ObjectiveMain objective: To review systematic reviews of the efficacy of behavioral interventions to prevent STIs and unintended pregnancies.
Secondary objectives: To assess differences in behavioral intervention results according to their use of objective and subjective outcome measures; to study differences in Cochrane and non-Cochrane Collaboration review findings.
MethodsInclusion CriteriaWe included systematic reviews and meta-analyses that 1) evaluated sexual behavioral interventions aimed at preventing unintended pregnancies and/or STIs; 2) included more than 1 randomized clinical trial (RCT); 3) had high rates of controlled trials among the reviewed studies (two-thirds of the titles); 4) reported outcomes based on biological markers and/or behaviors; 5) were published in a peer-reviewed journal in 2000 or later; and 6) used an appropriate search strategy (articles indexed by DARE, Database of Abstracts of Reviews of Effects12).
The first 2 criteria established a minimum quality threshold for systematic reviews without excluding too large a number of titles published in recent years. In any case, we also did a secondary analysis of the group of systematic reviews that met the quality criteria of the Cochrane Collaboration, which generally only include RCTs, thus excluding trials without control groups. The Cochrane Collaboration itself monitors their own systematic reviews to ensure quality. By excluding non-Cochrane-method reviews from this analysis, we were removing those that could be expected to be twice as likely to report results favorable to the intervention.13
Types of InterventionsWe considered any type of behavior modification intervention to be of interest, whether based on counseling, provision of information (about pregnancy or STIs), or persuasion (meant to encourage condom or contraceptive use, abstention from or postponement of sexual relations, or decrease in the number of partners, etc.). We did not include reviews of studies assessing knowledge, attitudes, intentions, adherence to HIV therapy, or behavioral interventions targeting risk activities unrelated to sexual activity (e.g., intravenous drug use). Also excluded were reviews of studies on contraceptive injections or circumcision because they were not directly related to the effects of a sexual behavioral intervention. Nor did we include reviews of studies that evaluated interventions targeting domestic violence. Finally, we also set aside studies of interventions carried out only online or that paid fees for participation.
Types of Outcomes- -
Objective outcomes were those based on biological measures such as markers of semen exposure or the results of STI testing. The first draft of this review only included studies that used pregnancy tests to detect unintended pregnancies. However, nearly all the systematic reviews used data from birth and abortion rates or self-reports of pregnancy; therefore, we decided to include data from these reviews in our overview.
- -
Subjective outcomes comprised any change in sexual behavior described by the participants or investigators. Examples are the reported use of condoms at set intervals, number of partners, or STI symptoms. We excluded information that did not refer to specific acts or behaviors.
Two authors (A.M.P. and A.C.S.) undertook a literature search not limited by language in April 2015. A series of search terms (see supplementary material) were introduced into the following databases: EMBASE, MEDLINE, Cochrane Library, PubMed, Psycinfo, and Google Scholar. We also consulted the System for Information on Grey Literature in Europe (SIGLE) and hand searched journals.
Data Collection and AnalysisThe 2 authors searched independently for eligible systematic reviews. A template for data collection covered the following information: type and number of participants, intervention, and items on the AMSTAR checklist (for Assessing the Methodological Quality of Systematic Reviews; whether or not the reference was a Cochrane review (or a Cochrane-method review); comparators and outcomes; and subgroup analyses. One author (A.M.P.) introduced the data and a second (A.C.S.) checked accuracy. If doubts arose, they were resolved through the consensus of all 3 authors (including J.R.F.R.).
Evaluation of the Methodological Quality of the Included ReviewsThe AMSTAR score was used to assess systematic review quality.
The GRADE scale (for Grading of Recommendations Assessment, Development and Evaluation) was used to record the evidence level provided.
We also checked whether the reviews evaluated the heterogeneity of included trials (χ2<0.1 or I2 statistic: average heterogeneity, 50%; high heterogeneity, >75%). We recorded whether meta-analyses included an assessment of publication bias (with funnel plots for example).
Data SynthesisMeta-analysis was not possible because of the heterogeneity of interventions, participants, follow-up periods, and types of outcome. We also found that data were sometimes unavailable or that some reviews overlapped. Therefore, we decided on a descriptive, narrative analysis of the findings of the systematic reviews and interpreted them as clearly and simply as possible in the interest of aiding clinicians and health policymakers’ decisions. Each systematic review was classified according to the level of evidence that an intervention had produced a real effect on STIs or unintended pregnancies.
The reviews were first classified qualitatively for analysis as follows:
- 1.
Reviews that looked at objective, or biological, outcomes and that preferably had included studies that also used objective measures.
- 2.
Reviews that had included studies assessing subjective outcomes (self-reports of condom use during recent sexual intercourse and at other intervals, STI symptoms, number of partners, age of onset of sexual activity).
From each group, we selected the number of studies that supported a given outcome. We recorded the statistic each systematic review used for comparisons (odds ratio, relative risk, effect size [Cohen's d]). If absolute numbers on which calculations were based were given in the reviews, we recorded them, and analyzed heterogeneity (χ2, I2 index, Q statistic).
Along with our analysis of the reviews’ findings for objective vs subjective outcomes, we summarized the findings of each systematic review in the following terms:
- -
“Effect” if a meta-analysis found that the behavioral intervention had a statistically significant effect, or in the absence of meta-analysis, if most of the included studies reported significant effects.
- -
“No effect” if a meta-analysis found that the behavioral intervention had no significant effect on outcomes, or in the absence of meta-analysis, if most of the outcomes reported by the included trials reported no significant effects.14
- -
“Indeterminate” if the proportions of positive and negative outcomes were similar, including cases in which meta-analysis could be done on only some of the outcomes.
As suggested in the PRISMA guidelines (listing the Preferred Reporting Items for Systematic Reviews and Meta-Analyses), we prepared a flow chart of the literature search that specifies excluded articles (see supplementary material). Of the 9765 titles initially found, we finally included 55 systematic reviews.
Description of the Included Systematic ReviewsThe included reviews evaluated interventions based on various strategies applied in different age brackets and settings. They bring together data for a heterogeneous population (men who have sex with men, HIV-positive persons, sex workers and their clients, truckers, students, homeless young people, young prisoners, elderly persons living in geriatric facilities, individuals in countries with both low and high per capita income levels, psychiatric patients, and more). Many clinical trials were included in more than one systematic review.
Quality of the Included TrialsThe methodological quality of the systematic reviews was high on the whole; however, the quality of the trials they included was moderate (see supplementary material).
Nearly all the systematic reviews analyzed the scientific quality of the included trials. They also commented on possible conflicts of interest and risk of publication bias. The greatest variability affected the inclusion criterion referring to type of study: many reviews included nonrandomized trials, pre-post intervention studies, cross-sectional and other observational studies, or they did not make clear the number of such studies they included. Such heterogeneity affects a review's results. More nonrandomized trials have been included in recent years. Authors often present tables with detailed descriptions of the included titles but do not give details of their specific findings.
Authors that undertook a meta-analysis of the data usually found that the level of heterogeneity was high.
None of the systematic reviews used exclusively objective outcome measures to study changes in sexual behaviors. All the reviews we included mentioned the risk of bias in self-reports of behaviors.
Outcomes of InterventionsOur findings cannot be analyzed quantitatively, given that the interventions, measurement intervals, and populations in the studies included in the reviews were heterogeneous. Many studies were included in several systematic reviews. Table 1 shows the outcomes of behavioral interventions for each systematic review; statistical results can be found in the supplementary material. We can say that 29 of the 40 reviews (72.5%) that evaluated objective data for pregnancies and/or STIs found no positive effect of the behavioral interventions in exposed vs control subjects. Two reviews concluded that an effect could not be determined (“indeterminate”), and 9 (22.5%) detected some effect but it was generally marginal.
Systematic Reviews of Sexual BIs and Their Main Findings.
| Systematic Review | Objective Outcomes | Effect of BIa | Subjective Outcomes | Effect of BIa |
|---|---|---|---|---|
| Althoff et al. (2014)32 Women from Latin America, United States | MTA and 1/3 RCT, yes ↓ incidence of nonviral STIs. | Yes | MTA and 3 RCTs, yes ↓ in risk behaviors; 1 RCT, no ↓. | Yes |
| Bennet and Assefi (2005)16 Adolescents, schools | 2 RCTs, no ↓ in unintended pregnancies. | No | 7/11 RCTs, no postponement of age of onset of SXR; in 3 RCTs, yes postponement of SXR, but in 1 RCT, SXR were brought forward; 6/11 trials, no ↓ in SXR (4 ↓ and 1 ↑); 7/11 RCTs, no ↓ in no. of partners; 4/5 RCTs, no ↑ in condom use; 6/11 trials, yes ↑ in contraceptive use, in 4 no change, in 1 ↓. | No |
| Berg et al. (2011)56 MSM | 1 RCT, no ↓ in HIV incidence; 1 RCT, no ↓ in STI incidence. | No | 2 RCTs and MTA, no ↑ in condom use (in anal sex with usual partner); 2 RCTs and MTA, no ↑ in condom use (in anal sex with occasional partners). | No |
| Blank et al. (2012)17 <25 y | 6/7 studies, no ↓ in unintended pregnancies; 1 trial, no ↓ in STI rate. | No | 7 studies, no ↓ in sexual risk behaviors, but in 1, yes ↓. | No |
| Burton et al. (2010)57 | 2 studies, no ↓ in STI rate. | No | 3 studies, yes ↑ in condom use; 1 study, no ↑ in condom use. | Yes |
| Couples | ||||
| Ferreira et al. (2009)58 ♀ after abortion | Not evaluated | – | MTA and 2/3 RCTs, no ↑ in contraceptive use 4 mo after abortion. | No |
| Carvalho et al. (2011)59 ♀ HIV+ | 1 trial, yes and 1 trial no ↓ in infections (Chlamydia, gonorrhea, trichomoniasis) at 3 mo. | Indeterminate | MTA and several trials, no ↑ in consistent condom use at 3, 6 or 12 mo. | No |
| Chin et al. (2012)18 Adolescents | MTA and trials, no ↓ in unwanted pregnancies after all BI types; MTA and trials, yes ↓ in STIs after comprehensive risk interventions; MTA and trials, no ↓ in STIs in abstinence programs. | No | Improvement in no. of partners and condom use with comprehensive risk interventions, but not with abstinence programs. | Indeterminate |
| Crepaz et al. (2006)37 PLWHIV | 1 RCT, no ↓ in Chlamydia infection or gonorrhea in HIV+ MSM; 1 RCT, yes ↓ in Chlamydia infection and gonorrhea in VIH+ ♀; MTA, yes ↓ incidences of Chlamydia infection and gonorrhea. | Yes | MTA and 5/12 trials, yes ↑ in condom use. | Yes |
| Crepaz et al. (2007)33 Blacks and Latin Americans in clinics | MTA and 4/13 RCTs, yes ↓ in STI rates. | Yes | MTA and 4/12 RCTs, yes ↑ condom use. | Yes |
| Crepaz et al. (2009)34 African Americans in USA | MTA and 4/17 trials, yes ↓ in STIs; 13/17 trials, no ↓ in STI rates. | Yes | MTA and 13/33 trials, yes ↓ in risk behaviors related to HIV. | Yes |
| Darbes et al. (2008)41 African American HTXs | MTA of 10 RCTs, no ↓ in STI incidence. | No | MTA and 10/38 trials, yes ↑ in condom use; 28/38 trials no ↑ in condom use. | Yes |
| DiCenso et al. (2002)19 <18 y | MTA and 12 trials, no ↓ in pregnancy rates; MTA and 5 trials, ↑ in pregnancies in partners of ♂. | No | MTA and many trials, no postponement in onset of SXR or ↑ in contraceptive use in most recent intercourse in ♀ or in ♂. | No |
| Fonner et al. (2012)14 Developing countries | MTA and 3/3 trials, no ↓ in HIV incidence; 1 trial, ↑ in HIV incidence; 2 trials, no ↓ in STI rates; and 1 trial, yes ↓ in STI rate but based on self-reported symptoms; 2 trials, no results reported. | No | MTA and 14 trials, no ↑ in condom use; on analysis by subgroups, no effect in ♂or ♀, but yes in HIV+ individuals; MTA, 5 studies, yes ↓ in no. of partners; MTA of subgroups; and 3/5 trials, no effect (♂, ♀, or HIV+ individuals). | No |
| Fonner et al. (2014)30 Universities in countries with low-middle incomes | Not evaluated | – | MTA and 3/10 studies, yes ↑ in condom use; MTA and 5/6 trials, yes postponed onset of SXR; MTA and 1/4 trials, yes ↓ in no. of partners; 8 trials, yes, improved self-efficacy (using condoms and avoiding SXR). | Yes |
| Henny et al. (2012)35 | Yes, ↓ STIs. | Yes | MTA, yes, effect on condom use. | Yes |
| African Americans HTX | ||||
| Herbst et al. (2005)60 MSM | Not evaluated | – | MTA of 29 studies, yes ↓ in unprotected anal sex; 19/23 trials, no ↓ in unprotected anal sex; MTA and 10 studies, no ↓ in no. of partners MTA and 4 studies, no ↓ in unprotected oral sex | Indeterminate |
| Herbst et al. (2007)61 Latin Americans in USA | MTA of 3 RCTs, no ↓ in STI incidence.b | No | 19 trials, yes ↓ in sexual risk behaviors (any analyzed); 11 trials, yes ↑ in consistent condom use; 8 trials, yes ↓ in no. of partners. | Yes |
| Herbst et al. (2007)62 MSM | 1 trial, no ↓ in HIV incidence at 12 or 18 mo; 1 trial, no ↓ in bacterial STIs at 12 mo; 1 trial, borderline statistical effect on “new STIs” at 12 mo. | No | Individual BIs: MTA of 6 BIs, yes ↓ in unprotected anal sex. Group BIs: MTA of 15 trials, yes ↓ in unprotected anal sex. Community BIs: MTA of 6 trials, yes ↓ in unprotected anal sex. 3 types of BI: no ↓ in no. of partners or unprotected oral sex. BIs not entered into MTA: 41/57 trials found no effect. | Yes |
| Lu et al. (2013)11 MSM in China | MTA of 6 trials, no ↓ in prevalence of syphilis (in 2 trials ↑ in syphilis in the intervention group); MTA and 3/10 trials, ↑ in HIV prevalence; 7/10 trials, no ↓ in prevalence. | No | 7/25 trials, yes ↑ in consistent condom use; 8/10 trials, yes ↑ in HIV testing. | Yes |
| Johnson et al. (2006)63 PLWHIV | Not evaluated | – | MTA and 3/19 trials, yes ↑ in condom use; MTA and 7/7 trials, no effect on no. of partners. | Indeterminate |
| Johnson et al. (2008)64 MSM | Not evaluated | – | BI vs no intervention: MTA of 40 trials, yes, effect. BI in small groups: MTA and 1/18 RCTs, yes ↓ in unprotected SXR. Individualized BIs: MTA and 11/11 RCTs, no ↓ in unprotected SXR. Community interventions: MTA and 1/10 RCT, yes effect. Comparison between BIs: MTA and 2/18 trials, yes ↓ in unprotected SXR. | Yes |
| Johnson et al. (2009)65 African Americans in USA | MTA, yes ↓ in STI rate. | Yes | MTA, yes ↑ in condom use (slight effect: Cohen's d for mean effect sizes 0.12); MTA, no ↓ in no. of partners. | Indeterminate |
| Johnson et al. (2011)15 Adolescents | MTA, yes ↓ in STI incidence. | Yes | Weighted average of effect size: no ↑ in overall use of condoms in SXR in general or in anal intercourse, but yes ↓ in no. of partners, and yes postponement of onset of SXR. Effect size of effect on frequency of SXR: effect of BI with no abstinence focus, but only in institutionalized. | Indeterminate |
| Kennedy et al. (2013)66 ♀ (+1 in orphans and 1 in young people) | Not evaluated | – | Microcredits: 2 trials, no ↑ in condom use in most recent SXR. Microcredit+education: 1 study, no ↑ in condom use; 1 trial study, yes ↑ in condom use in ♂ but not in ♀. Microcredit+health education+job training: 3 studies, no ↑ in condom use or ↓ in no. of partners. Job training+health education: 2 trials, no ↑ in condom use. | No |
| Kirby et al. (2007)20 Education, young people | 9/13 trials, no ↓ in pregnancy rate; 3/13 trials, yes ↓; and 1/13 trials, ↑; 6/10 trials, no ↓ in STI rate; 2/10 trials, yes ↓; and 2/10 trials, ↑ in STI rate. | No | 29 (55%) did not postpone SXR, 22 (42%) postponed, and 1 (3%) brought SXR forward; 19 (61%), no ↓ in SXR frequency; 9 (29%) yes ↓; and 3 (10%) ↑; 21 (62%), no ↓ in no. of partners, 12 (35%) yes ↓, and 1 (3%) ↑; 28 (52%), no ↑ in condom use, 26 (48%) yes ↑; 8/15 trials, no ↑ in contraceptive use, 6 yes ↑, and 1 ↓ in contraceptive use. | No |
| Kirby (2008)67 Contraception in adult ♀ | 5/5 trials, no ↓ in unintended pregnancies; 1 trial, no ↓ in abortions; 4/4 trials, no ↓ in STIs. | No | 5 trials, no ↑ in condom use overall; 3 trials, yes ↑ in contraceptive use but 2 trials, no ↑. | No |
| Lazarus et al. (2010)27 Young people, aged 10–24 y in Europe | Not evaluated | – | BIs delivered by teachers: 5 studies, no ↑ in condom use or other variables; BIs delivered by counselors: 10/11 trials, no improvement in sexual behaviors; BIs delivered by health care professionals: 7 trials, no change in sexual behaviors. Others (HIV+ young people, subjects in clinics, in schools): 16 trials, no improvement in sexual behavior. | No |
| Lopez et al. (2010)68 ♀ <1 mo postpartum | 3 RCTs, no ↓ in unintended pregnacies 1 RCT, yes ↓ in pregnancies at 18 mo | No | Short-term counseling: 1 RCT, no ↑ in contraceptive use at 3 mo, but yes at 6 mo; 2 RCTs, no ↑ in contraceptive use at 1 y; 1 RCT, yes ↑ at 8–12 wk. Programs with multiple contacts: 1 RCT, yes ↑ in contraceptive use at 6 mo, 1 RCT no ↑ at 4 mo; | Indeterminate |
| Lopez et al. (2013)69 ♀, excluding individuals “at risk” | 10/12 RCTs, no ↓ in pregnancy rate; 2/12 RCTs, yes ↓ in pregnancy rate (1, self-reports; 1, home visits) | No | 6/10 trials, no ↑ in any contraceptive use at 1–24 mo; 12/20 trials, no ↑ in condom use at 6–36 mo. | No |
| Lopez et al. (2013)70 HTX | 5/5 trials, no ↓ in pregnancy rate; 4/4 trials, no ↓ in HIV incidence or prevalence; 2 trials, no ↓ and 2 trials yes ↓ in rate of HSV-2 infection; 1 trial yes and 2 trials no ↓ in syphilis prevalence; 2 trials no ↓ (or ↑) in prevalence of gonorrhea or Chlamydia infection; 1 trial no ↓ prevalence of trichomoniasis at 3 y. | No | Not evaluated | – |
| Lopez et al. (2014)71 HTX | Computer-mediated intervention, adapted vs unadapted: 1 RCT, no ↓ pregnancy or STI rates in ♀ at 2 y. Counseling+telephone calls vs counseling alone: 1 trial, no ↓ in unintended pregnancy or STI rates in ♀ at 12 mo. Counseling vs standard intervention: 1 trial, no ↓ in unintended pregnancy or STI rates in ♀. | No | Counseling+phone vs counseling: 1 RCT, no ↑ in dual contraceptive use at 3 or 12 mo. Counseling vs standard care: 1 RCT, no ↑ in dual contraceptive use at 3 or 12 mo. | No |
| McCoy (2009)72 ♀ in low-to-middle- income countries | 9 studies, no ↓ in the incidence of HIV; in 2 trials studies yes ↓; 3 studies, no ↓ in syphilis, Chlamydia infection, or gonorrhea rates; 3 studies, no ↓ in HSV-2 infection but in 1 study, yes ↓; 1 trial, yes effect on the variable “any STI.” | No | 7/10 studies, yes ↓ in sexual risk behaviors; 3/10 studies, yes effect in some subgroups (clients of sex workers, occasional partner). | No |
| Meader et al. (2010)43 Drug addicts | Not evaluated | – | MTA, no effect on comparing psychosocial BIs vs standard education vs minimal intervention controls; yes, effect on comparing multisession psychosocial BI vs minimal intervention controls. | No |
| Meader et al. (2013)44 Drug addicts | Not evaluated | – | MTA and 6/46 trials, yes ↑ in condom use and protected sex (BI vs education); MTA and 3/7 trials, yes ↑ in condom use and protected sex (BI vs minimal or no BI). | Yes |
| Michielsen et al. (2010)21 Sub-Saharan youth | MTA and trials, no ↓ in HIV rate 1 trial, ↑ in prevalence of gonorrhea in the intervention group; 1 RCT, no ↓ in prevalence of Chlamydia infection, syphilis or HSV-2; yes, ↓ in HSV-2 (but not in ♂ or ♀ when analyzed separately). | No | MTA and 2/9 trials, yes ↑ in condom use in last SXR only in ♂. In ♀, no ↑ (data not reported) MTA, yes ↑ in condom use “in general or sometimes.” In ♀ and in the general population, no ↑ (data not reported). | Yes |
| Moreno et al. (2014)39 All group types | MTA and all RCTs included found no effects on the incidence or prevalence of HIV, syphilis, HSV-2, gonorrhea, Chlamydia infection, trichomoniasis or a composite biological score outcome (see supplementary material). | No | MTA and 3 RCTs, yes ↑ in condom use (in recent SXR); 1 RCT, no ↑ in condom use (in recent SXR with occasional partners); 1 RCT, no ↑ in condom use with usual partner of last 3 y; 1 RCT, no ↑ in consistent condom use over 6 mo and nearly identical negative results at 12 and 24 mo; MTA and 5 RCTs, no ↓ in no. of partners for those reporting ≤2 in last year. | No |
| Mullen et al. (2002)22 Adolescents (sexually active) | MTA and trials, no ↓ in STI rates. | No | MTA and trials, yes ↓ in no. of unprotected SXR trials, no ↓ in no. of partners. | Indeterminate |
| Naranbhai et al. (2011)28 Homeless youth | Not evaluated | – | 1 RCT, no effect in ♂ on no. of partners, frequency of unprotected SXR at 3 or 24 mo), but yes effect on ♀; 1 RCT, no effect on a 7-item scale; 1 RCT, no ↓ in no. of partners at 1 d or 3 mo and no ↑ in condom use. | No |
| Neuman et al. (2002)36 HTX couples in USA | MTA and 3/6 trials, yes effect. | Yes | MTA, yes ↑ in condom use and yes ↓ in unprotected SXR; MTA, no ↓ in no. of partners; MTA and 3/11, improvement in risk behaviors. | Yes |
| Ojo et al. (2011)73 Risk occupations (truck drivers, migrants, military personnel, tourism industry workers) | VCT: 1 RCT, no ↓ in HIV incidence. Education-training vs alternative education: 1 RCT, yes ↓ in STI incidence. | Indeterminate | VCT vs no VCT: 1 RCT, yes ↓ in self-reported STI symptoms; 1 RCT, no ↓ in no. of unprotected SXR or SXR with sex workers; 1 RCT, yes ↓ in unprotected SXR with sex workers. Education vs no intervention: 1 RCT, yes ↓ in unprotected SXR; 1 RCT, no ↓ in no. of partners. Education-training vs alternative education: MTA and 1/3 RCTs, yes ↓ in unprotected SXR; 1 RCT, no ↓ in unprotected SXR with sex workers; MTA and 2/3 RCT, no ↓ in no. of partners. | No |
| Oringanje et al. (2009)23 Adolescents (10–19 y) | Multiple interventions: MTA and 2 RCTs of individualized BIs, no ↓ in risk for unintended pregnancy; MTA and 5 RCTs, no ↓ in risk for unintended pregnancy; 1 RCT, no ↓ in no. of births; 1 RCT, no ↓ in risk for 2nd unintended pregnancy. Contraceptive use: 1 trial, no ↓ in STIs. Encouragement to use contraceptives: 2 RCTs, no ↓ in risk for unintended pregnancy; 2 RCTs, no ↓ in risk for STIs. | No | Multiple interventions: no effect on the use of condoms in recent SXR, on consistent use of condoms, on oral (hormonal) contraceptive use, on age of onset of SXR (RCTs enrolling clusters); yes, effect on age of onset of SXR in RCTs enrolling individuals. Educational interventions: no postponement of onset of SXR; yes ↑ in condom use in recent SXR. Encouragement to use contraceptives: no effect on age of onset of SXR, condom use in recent SXR, consistency of condom use, or use of emergency contraceptives; yes ↑ in oral contraceptive use. | No |
| Ota et al. (2011)74 Sex workers and clients in high-income countries | 2 RCTs, no ↓ in STI incidence | No | 1 RCT, no ↑ in condom use; 1 RCT, no ↑ in condom use in 26 clients of sex workers; 1 RCT, yes ↓ in self-reported STIs in clients of sex workers. | No |
| Pandor et al. (2015)75 Psychiatric patients | Not reported | – | 5 trials, no ↓ in no. of partners; 2 RCTs, yes effect; 3 trials, no ↓ in no. of unprotected SXR; 3 trials, yes, ↓. | No |
| Picot et al. (2012)29 Adolescents in school | Not reported | – | MTA and 3/5 RCTs, no postponement of onset of SXR; MTA and 13/15 RCTs, no ↑ in condom use; 6/6 RCTs, no ↓ in no. of partners (but ↓ in anal sex in 1 subgroup). | No |
| Scott-Sheldon et al. (201042 Patients of STI units | MTA, no ↓ in STI incidence in the short term, but yes ↓ in the medium-to-long term. MTA and trials, yes ↓ in HIV incidence over the long term. | Yes | No long-term ↑ in condom use, but yes, short-term ↑; only short-term ↓ in no. of partners. | Indeterminate |
| Schnall et al. (2014)76 MSM | Not reported | – | Text messages and emails: 1 trial, no effect on condom use. Video games: 1 trial, no effect on condom use. Online program “Keep It Up!”: yes, effect at 12 wk. | No |
| Shepherd et al. (2011)77 ♀, cervical cancer prevention | Comparison 1, BI vs basic intervention: 3/4 trials, no ↓ in Chlamydia. In all trials, no ↓ gonorrhea, trichomoniasis, or inflammatory pelvic disease. Comparison 2, BI vs general health education: 1 trial, ↑ or ↓ in Chlamydia, depending on analytical method (incidence/100 person-years vs regression modeling); 1 trial, no ↓ in trichomoniasis or gonorrhea. Comparison 3, BI vs BI (a different one by another supplier or medium): 1 trial, yes ↓ self-reported Chlamydia symptoms, but no effect when confirmed clinically; 1 trial, ↓ in self-reports of a set of STIs. Comparison 4, BI vs no intervention: no trials found. | No | Comparison 1: 2/6 trials, yes ↑ in condom use (at 6–12 mo); 2/6 trials, no ↑ at 2 y; 2/6 data not reported; 4/5 trials, no ↑ in condom use in recent SXR. Comparison 2: 7 comparisons with similar nos. of trials finding and not finding an effect on condom use in recent SXR at 6 or 12 mo (see supplementary material). In all trials, no ↓ in no. of partners or overall activity. Comparison 3: no change in condom use or activity. Comparison 4, BI vs no intervention: no ↑ in condom use, no. of protected SXR, or no. of ♀ abstaining; yes ↓ in no. of partners. | Indeterminate |
| Tolli et al. (2012)26 <25 y, in Europe | 1 RCT, no ↓ in abortions or no. of births. | No | 1 RCT, no ↓ in self-reported STIs; 3 trials, no ↑ in condom use; 1 trial, no ↓ in no. of partners. | No |
| Tolou-Shams et al. (2010)31 Adolescents in prison | Not evaluated | – | 5/8 trials, very modest effect size (Cohen's d, 0.18; range, 0.09–0.28); 4/8 RCTs, no effect. | Yes |
| Townsend et al. (2013)51 HTX ♂ in low-to-middle income countries | Not evaluated | – | 9 studies, yes ↑ in condom use; 3 studies, mixed results; 6 studies, no effect. 7 trials, no ↓ in no. of partners; 4 trials, yes ↓; 2 trials, mixed results. | Indeterminate |
| Underhill et al. (2007)24 Youth in USA | 8/8 trials, no ↓ in pregnancies; 9/9 trials, no ↓ in STIs. | No | 7/7 RCTs, no ↓ in self-reported STIs; 5/5 RCTs, no ↓ in no. SXR. Other results: no ↓ in age of onset of SXR or vaginal sex, or change in condom use (13 comparisons in all). | No |
| Underhill et al. (2008)25 Youth in USA | 3 RCTs, no ↓ in rates of self-reported STIs; 7 RCTs, no ↓ in unintended pregnancy rate. | No | 12 analyses of various outcomes (unprotected anal, oral or vaginal sex): similar nos. of RCTs finding and not finding an effect (see supplementary material); 9 RCTs, no ↓ in partners but 4 RCTs, yes ↓; 15 trials, no effect on postponing onset of SXR but 4 trials, yes an effect; | Indeterminate |
| Ward et al. (2005)40 Patients in STI units | MTA and 7/8 RCTs, no ↓ in STIs; MTA and 3/3 RCTs, no ↓ in clinically diagnosed STIs. | No | 1/2 RCTs, no ↓ in STIs but 1 RCT, yes ↓; MTA and 2/7 RCTs, yes ↑ in consistent condom use. | Indeterminate |
| Wariki et al. (2012)78 Sex workers and clients in low-to-middle income countries | Social-cognitive therapy vs standard counseling: 1 trial, no ↓ in the HIV, syphilis, gonorrhea, Chlamydia infection or any STI incidence at 6 mo. Community empowerment vs standard intervention: 1 trial, no ↓ in the prevalence of syphilis at 6 mo; 1 trial, yes ↑ in the prevalence of HSV-2 at 6 mo. Peer education+clinic-based counseling vs peer education alone: 2 RCTs, no ↓ in the prevalence of Chlamydia infection, gonorrhea, trichomoniasis, or any STI at 12 or 18 mo; 1 RCT, yes ↓ on the prevalence of Chlamydia infection at 6 mo. Encouragement to use female and male condoms vs encouragement to use male condom only: 1 trial, no ↓ in the incidence of VIH, Chlamydia, or gonorrhea. Intensive STI screening vs basic screening: 1 trial, no ↓ in the incidence of HIV or prevalence of gonorrhea or trichomoniasis at 6 mo, but yes ↓ in prevalence of Chlamydia. | No | Social-cognitive therapy vs standard counseling: no effect on condom use at 1 or 6 mo; no effect on SXR with regular or occasional partners; no ↓ in sexual activity; yes ↑ in consistent condom use at 6 mo. Social-cognitive therapy vs no intervention: 1 RCT, no ↑ in consistent condom use at 7 d or 6 mo. Community empowerment vs standard intervention: 1 RCT, yes ↑ in consistent condom use with regular clients; 1 RCTs, no ↑ in condom use with clients; 1 RCT, yes 100% ↑ in condom use at 6, 11, and 16 mo. Encouragement to use female and male condoms vs encouragement only to use male condom: 1 RCT, yes ↑ in mean use at 6 mo. Encouragement to use both female and male condoms vs encouragement only to use male condom: 1 RCTs, yes ↑ in combined use. VCT vs standard intervention on STIs: 1 RCT, yes ↑ in consistent condom use. | Indeterminate |
Abbreviations: BI, behavioral intervention; HSV, herpes simplex virus; HTX, heterosexuals; MSM, men who have sex with men; MTA, meta-analysis; PLWHIV, people living with human immunodeficiency virus; RCT, randomized clinical trial; STI, sexually transmitted infection; SXR, sexual relations; VCT, voluntary counseling and testing.
Effect means a statistically significant one (or not); such an effect does not necessarily indicate there is a true effect.
A positive effect was found when the data were analyzed with a pooled odds ratio assuming a fixed-effects model (i.e., with the presumption of an effect); however, when a random-effects model was used, there was no effect.79
No clear evidence emerged in 26 of the 54 reviews that looked at whether behavioral interventions modified sexual conduct with regard to subjective (self-reported) outcomes (e.g., condom use, number of partners, age of onset of sexual relations). Thirteen reviews (24%) concluded that the results of interventions could not be determined, but 16 (29.6%) did find evidence that the behavioral interventions had had an effect.
The absence of effect was most marked in young people and adolescents, who are the population groups most often named in these systematic reviews. Only 1 review among those that examined objective outcomes detected an effect.15 Eleven reviews could find none.16–26 Among the reviews that examined subjective outcomes, 9 out of 14 found that the interventions had no effect,16,17,20,23,24,26–29 3 found a positive effect,21,30,31 and 2 could come to no conclusion (“indeterminate”).22,25
Moreover, in the systematic reviews that did find an effect, which were a minority, the effect size was small. The authors of 6 of the 9 reviews reporting an effect estimated effect sizes that were near the statistical limit of significance or found that the intervention affected only some of the outcomes.32–37
The effect size detected in the relatively few systematic reviews that found an effect on subjective outcomes was also low (see supplementary material for the full set of results). Johnson et al.38 reported a relative risk (RR) of 0.73 (95% CI, 0.63–0.85) for unprotected anal sex in the intervention group, a figure that reflected a mean overall reduction in number of unprotected sexual encounters relations (from 10.1 to 7.4 at 6 months) and a reduction in the mean number of partners from 1.2 to 0.9.
Moreno et al.39 reported a statistically significant effect for only 1 of their 16 analyses, specifically an increase in condom use during recent sexual intercourse with any type of partner (RR=1.20; 95% CI, 1.03–1.40). The statistical significance is attributable to the fact that 255 of 961 participants reported using condoms after the intervention (vs 207 of 937 in the control group).
A systematic review by Ward et al.40 reported that 1163 of 2761 participants used condoms after behavioral interventions (vs 966 of 2700 participants in the control group). These figures mean that there was a RR of 1.17 (95% CI, 1.10–1.25) for this outcome and that the interventions had not changed the self-reported behaviors of 57% of the participants.
Oringanje et al.23 found no evidence of lower rates of unintended pregnancies or STIs in a meta-analysis of 41 RCTs enrolling a total of 95 622 adolescents. They did detect a certain degree of postponement of the onset of sexual relations (RR=0.86; 95% CI, 0.77–0.96), based on finding that 308 of 844 adolescents initiated sexual relations after the behavioral intervention in contrast with 331 out of 702 in the control group. Thus, two thirds of the participants did not change their behavior, according to self reports; moreover, the pregnancy and STI rates were similar in the intervention and control groups.
We observed marked differences between the findings of studies that used objective outcome measures and those that relied on self reports. Sixteen systematic reviews found evidence that behavioral interventions are effective when outcome data were from participants’ reports (Table 1). In contrast, 10 of the 16 reviews did not detect effects of the same interventions on the basis of objective outcomes; the difference is probably attributable to self-report bias.
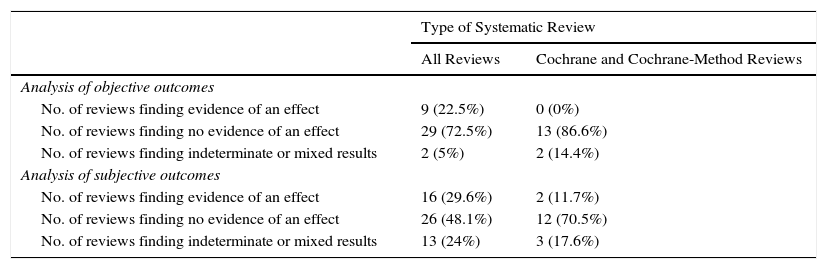
A trend toward absence of evidence of effect is greater in reviews that included higher-quality trials. The results of Cochrane reviews (or others that applied the same method) showed no evidence of effect on objective outcomes (13/15 reviews; 86.6%) or subjective ones (12/17; 70.5%). The remaining reviews reported uncertain results (3 references) or positive ones (2 references) (Table 2).
Synthesis of the Findings of the Systematic Reviews Included in This Overviewa
| Type of Systematic Review | ||
|---|---|---|
| All Reviews | Cochrane and Cochrane-Method Reviews | |
| Analysis of objective outcomes | ||
| No. of reviews finding evidence of an effect | 9 (22.5%) | 0 (0%) |
| No. of reviews finding no evidence of an effect | 29 (72.5%) | 13 (86.6%) |
| No. of reviews finding indeterminate or mixed results | 2 (5%) | 2 (14.4%) |
| Analysis of subjective outcomes | ||
| No. of reviews finding evidence of an effect | 16 (29.6%) | 2 (11.7%) |
| No. of reviews finding no evidence of an effect | 26 (48.1%) | 12 (70.5%) |
| No. of reviews finding indeterminate or mixed results | 13 (24%) | 3 (17.6%) |
See the supplementary material for the results for each behavioral intervention covered in each systematic review.
The tendency to find evidence of effect in poorer quality systematic reviews holds true when the results are analyzed by population subgroups receiving the behavioral interventions:
- -
Young people, adolescents, and students: None of the Cochrane (or similar) reviews detected an effect on interventions in this population.23–25,28
- -
African Americans: The higher quality reviews (Cochrane method, which only included RCTs with lower degrees of heterogeneity) found clearly negative outcomes of interventions.41 The other 2 systematic reviews relevant to this population included nonrandomized trials (1 in women and 1 in heterosexuals in general), finding that behavioral interventions did have an effect.34,35
- -
Patients attended in STI units: One systematic review that only included RCTs found no statistically significant effect of interventions overall.40 In contrast, a review that included studies without controls did find an effect on both objective and subjective results.42
- -
Drug addicts: A Cochrane review by Meader et al.43 found an absence of effect of interventions targeting risk behaviors related to STIs and HIV. When the same group published another review that included quasi-experimental studies, they did find a certain degree of evidence supporting an effect.44
Our results should be interpreted cautiously. The methodological quality of the systematic reviews we included was high, but the quality of the trials and other studies they examined ranged from low to moderate.
Some reviewers obtained different results when they meta-analyzed the findings of a portion of the included trials. Gathering data from different trials tends to exclude ones with divergent results.
Potential for Bias in the Review ProcessThe methods we used to search the literature, extract and synthesize the data, and evaluate methodological quality should have reduced the risk of bias in the present overview of systematic reviews. However, we may not have identified all the reviews published.
Our method for presenting the data from each systematic review facilitates the synthesis of findings and comparisons. We have presented nearly all the results from each trial included in each systematic review, thus avoiding the bias that sometimes arises when only the results of meta-analyses are considered, given that such analyses usually gather the results of only some of the studies the systematic reviews included.
The failure to demonstrate a statistically significant effect of a behavioral intervention does not imply that the intervention is ineffective; the sample size, for example, might have been inadequate. However, our main interest is to seek information about clinical usefulness that facilitates decision-making. Use of proper study designs could help demonstrate statistically significant effects for some behavioral interventions.
The comparator analyzed in some systematic reviews was not the absence of an intervention but rather a different type of behavioral intervention. If the control group had received no exposure to any type of intervention, the effects of the behavioral intervention of interest might have been statistically superior to the controls’ lack of exposure.
We could have chosen a different way to synthesize the results of each systematic review. However, we emphasize that evidence-based medicine prioritizes clarity of evidence and the practical usefulness of information. The aim is not to quantify an effect precisely but rather to find “evidence” of the type implied in the watchwords of the Cochrane Collaboration: trusted evidence, informed decisions, better health. Thus, we believe that other ways of synthesizing the information provided by each systematic review would have led to similar conclusions
Consistency Between StudiesHiga et al.45 carried out a review of the literature to identify why so few evidence-based behavioral interventions target homosexual behaviors. The authors found no evidence of improvements when they looked at biological outcomes (STIs, HIV infection). They also concluded that these interventions may be inadequate for achieving a real reduction in HIV infections.
The conclusions of other metareviews are quite similar: substantial effects are unsupported by objective results. Some authors have found that behavioral interventions “potentially” modify sexual behaviors based on subjective results, but even so the results are mixed or marginally significant.7,46–48
We concur with the opinion of Johnson et al.49 that the methodological quality of systematic reviews is high but that many quasi-experimental studies and even uncontrolled trials have been included in recent years. They found that “consumers of meta-analyses” do not compare the trials included in these analyses and that the real impact of published systematic reviews after 2009 (number of consultations on views in Google Scholar) has fallen drastically.
DiscussionWe were able to ascertain that 72.5% of the systematic reviews meeting our minimum quality criteria and published since 2000 failed to find evidence that behavioral interventions modify sexual behavior in general if the outcome is evaluated based on objective measures such as serology or pregnancy tests. A higher rate of Cochrane reviews (86.6%) failed to find such evidence.
When outcomes were assessed on the basis of self-reports, 48.1% of all systematic reviews and 70.5% of Cochrane reviews failed to find evidence that outcomes were better in the behavioral intervention groups than in controls.
If we consider only reviews that did find evidence of a statistically significant effect, we find that the results are far from optimal for effective prevention. The Cochrane Collaboration urges reviewers to select interventions to study with a view to providing information of value in making decisions about whether to use a particular intervention or not.50 An effect that is discretely superior to the control intervention's effect (which in any case is a result found in only a few studies and which in absolute terms can only be seen in a third of participants) does not seem to offer an optimal way to prevent STIs or unintended pregnancies.
The results of this overview are consistent with actual epidemiological figures, which do not show improvements in STI and unintended pregnancy rates in many countries in spite of the intense implementation of various ways of imparting sex education in schools and other settings.
We observed large discrepancies in findings according to the method used to assess the effect of the behavioral interventions chosen. In 10 of the 16 systematic reviews that did find evidence that an intervention affected sexual behaviors, the results based on subjective measures contradict the results based on objective ones. This is to say that when participants in the intervention group state that they used a condom or had fewer sexual partners than participants in the control group, their actual STI or pregnancy rate did not decrease below the level of the controls’. This pattern seems to show that their sexual behaviors did not in fact change and that self-reports are unreliable.
Self-reports are a source of bias for many reasons. For example, there is the propensity to give socially desirable responses, the influence of monetary incentives, availability of free condoms, use of psychoactive substances, and simple forgetfulness.31 For members of socially vulnerable groups (such as homeless persons, prisoners, sex workers, or students) there can be a motivation to offer positive answers to the researchers’ questions.51 For these and other reasons, results based on self-reports can be very different from those based on objective biological outcomes.
A telling example of this situation can be found in the systematic review of Ross et al.,52 which carried considerable weight in the various reviews we included. A systematic review by Fonner et al.30 included 21 RCTs evaluating condom use after various behavioral interventions, but data from only 8 of the 21 RCTs could be meta-analyzed, given the authors’ inclusion criteria. Only 3 of the included RCTs reported a statistically significant effect, yet in the meta-analysis showed that the intervention did have an effect. It was attributable, they stated, to the aforementioned systematic review of Ross et al., which had included 9645 randomized young people in 20 communities in Kenya between 1999 and 2002. That trial found noteworthy increases in condom use among men exposed to the intervention (RR, 1.47) but no effect on the incidence of HIV infection, 5 other STIs, or the rate of unintended pregnancy. Furthermore, when 7040 participants were reevaluated between 2005 and 2007, the previously identified effect had been eradicated.53 Therefore, a single finding in a subjective outcome in 1 RCT accounted for the positive result that was reported in the systematic review of Fonner et al., even though no objective positive outcomes were found and even though the effect disappeared over time.
These findings are consistent with a study that found that 42% of sex workers reported not having had sexual relations or having used a condom in their most recent intercourse, yet the presence of plasma prostate antigen in a vaginal smear demonstrated semen exposure.54
Quality control tools for studies do not currently distinguish between evidence from trials that assessed self-reporters rather than biological outcomes.
We conclude that it would be useful to consider possible steps to take in the interest of making real progress that will have an impact on the population:
- 1)
Designers of RCTs should use objective outcome measures, such as pregnancy tests or analyses for STIs, to study behavioral interventions.
- 2)
Developers of tools to evaluate the quality of RCTs and systematic reviews should consider distinguishing between subjective and objective outcome assessment measures.
- 3)
Educational policy-makers should promote interventions that are supported by evidence from high-quality RCTs showing a real (and large) effect based on objective measures of sexual conduct; this suggestion is consistent with recommendations from other overviews.46,55
- 4)
We should study interventions and policies implemented to manage other health problems for which real effects have been demonstrated; we should also examine educational strategies used in social groups with lower STI and unintended pregnancy rates.
The authors declare that no experiments were performed on humans or animals for this investigation.
Data confidentialityThe authors declare that no private patient data are disclosed in this article.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Albert Balaguer, Ramon Grimalt, María Jesús Barberà, Luis Álvarez.
Please cite this article as: Macaya Pascual A, Ferreres Riera JR, Campoy Sánchez A. Intervenciones conductuales para la prevención de infecciones de transmisión sexual y embarazo no deseado: revisión de revisiones sistemáticas. Actas Dermosifiliogr. 2016;107:301–317.


