






Since 2021, an increase in cases of tinea capitis has been detected in adolescents who shave their hair with fade haircut.
Patients and methodsMulticenter retrospective observational study of cases of cephalic pole dermatophytosis with a history of having been acquired after frequent shaving in hairdressing. A call was made to dermatologists from the Spanish Academy of Dermatology and Venereology (AEDV) to provide cases observed between January 2021 and December 2022. Patients with microbiological confirmation by culture or direct examination with KOH were included.
Results107 cases were collected, 106 of which were male. 78 non-inflammatory forms were observed, compared to 29 inflammatory. The most frequently isolated fungus was Trichophyton tonsurans (75.7% of cases). The lesions appeared predominantly on the nape of the neck and temporal area.
ConclusionsThe distribution by sex, age and lesional location seems to indicate that a new social trend, in which male adolescents regularly go to hairdressers to shave the occipital and temporal areas, would be the cause of this grouping of cases of ringworm of the scalp. The most frequent microorganism in our study (T. tonsurans) coincides with the most prevalent in our environment. This study shows an accumulation of cases that can be taken into account by competent Public Health agencies, which are responsible for ensuring compliance with the rules of disinfection of the material used for shaving.
Desde 2021 se ha detectado un aumento de casos de tiñas del cuero cabelludo en adolescentes que se cortan el pelo mediante rasurado o degradado.
Pacientes y métodosEstudio observacional retrospectivo multicéntrico de casos de dermatofitosis del polo cefálico con el antecedente de haber sido contraídas tras el rasurado frecuente en peluquería. Se realizó una llamada a dermatólogos de la Academia Española de Dermatología y Venereología (AEDV) para que aportaran casos observados entre enero de 2021 y diciembre de 2022. Se incluyeron pacientes con confirmación microbiológica mediante cultivo o examen directo con KOH.
ResultadosSe recogieron 107 casos, siendo 106 pacientes varones. Se observaron 78 formas no inflamatorias frente a 29 inflamatorias. El hongo aislado con mayor frecuencia fue Trichophyton tonsurans (75,7% de los casos). Las lesiones aparecieron predominantemente en la nuca y en el área temporal.
ConclusionesLa distribución por sexo, edad y localización lesional parece apuntar a que una nueva tendencia social, en la que adolescentes varones acuden asiduamente a peluquerías para el afeitado de las zonas occipital y temporal, sería la causante de esta agrupación de casos de tiña del cuero cabelludo. El microorganismo más frecuente en nuestro estudio (T.tonsurans) coincide con el más prevalente en nuestro medio. Con el presente estudio se evidencia un acúmulo de casos susceptible de ser tenido en cuenta por organismos competentes de salud pública, a los cuales corresponde velar por el cumplimiento de las normas de desinfección del material empleado para el rasurado.
Ringworm of the scalp, or tinea capitis, is a highly infectious disease that mainly affects children between 6 months and 12 years of age,1 with a slight predominance in boys.2 Depending on the route of transmission of the causative fungus of tinea capitis, we can distinguish 3 types of dermatophyte3: anthropophilic (including Trichophyton tonsurans, Trichophytonrubrum, Trichophyton interdigitale, Trichophyton violaceum, and Microsporum audouinii), which generally cause noninflammatory clinical forms; zoophilic (mainly Trichophyton mentagrophytes, Trichophyton verrucosum, and Microsporum canis), which usually cause inflammatory forms, and geophilic (Microsporum gypseum), causing moderate inflammation.
The pathogens responsible for tinea capitis vary over time and by geographic region studied. During 19th century and through to the middle of the 20th century, the dominant pathogen in Europe and the United States was the anthropophilic Microsporum audouinii,4 endemic in Africa,5 followed by the zoophilic M. canis.6 The use of griseofulvin, along with campaigns to identify and treat infection led to an increase in the prevalence of anthropophilic fungi from the middle of the 20th century, with less infections showing fewer clinical symptoms. Such fungi include T. tonsurans, which was endemic originally in Southeast Asia and Australia, before spreading to Central and South America, and from there to Europe and the United States.7 Currently, in the United States, this fungus is responsible for more than 90% of cases of tinea capitis, with a predilection for people of African origin, with M. canis being the second most common causative agent.3
In urban areas in Europe, the most common causative agents of tinea capitis are the anthropophilic species (in countries such as Spain, Belgium, or Poland), whereas other areas still have a predominance of zoophilic species, particularly M. canis (in countries such as Greece or Germany).8 Other studies, such as the one conducted in 2016 in Würzburg, Germany,9 showed that although M. canis remained the most frequent causative agent of ringworm of the scalp in that region, other anthropophilic fungi were gaining ground, most notably T. interdigitale.
Among the studies that report a high current prevalence of T. tonsurans in European countries and the Mediterranean basin, there are some conducted in Israel,4 and one published by Müller et al.,7 in which 18 young males had tinea capitis or tinea barbae caused by this dermatophyte up to 2 weeks after having had their haircut. We have also observed an increase in cases of ringworm caused by T. tonsurans in different parts of Spain in adolescent patients in our clinical practice since 2001. This apparent grouping of cases in time coincides with a new fashion among young Spaniards of shaving their head in the occipital and temporal area every week or twice a month. In light of this clinical observation, we decided to perform a study at the national level to analyze a series of cases of ringworm of the scalp associated with this new social trend.
Patients and methodsThis was an observational, retrospective, multicenter study of cases of dermatophyte infections of the head after a shave haircut at the hairdressers. The study was approved by the Ethics Committee for Drug Research of the Hospital General in Granollers (Barcelona, Spain) (number 2022.042). The cases were reported by dermatologists belonging to the Spanish Academy for Dermatology and Venereology during December 2022, after a call for participation via Dermachat.10
The inclusion criteria were microbiological confirmation by direct examination with KOH and/or culture, performed by obtaining sample by skin scraping in the dermatology clinic, and receipt of a shave haircut in a public hairdresser in the 2 weeks prior to the first visit to the clinic. Cases were identified from January 1, 2021, through December 31, 2022.
The variables collected were age, sex, site of initial lesion (back of the head/occipital, temporal/retroauricular, preauricular, facial, and others), spread to other areas, inflammatory versus noninflammatory ringworm, availability of direct examination and/or culture and corresponding result, accompanying clinical symptoms (swollen lymph nodes, fever, pain, others), prior treatments, treatments prescribed, and presence of subsequent indirect contagion.
ResultsOf the 883 dermatologists contacted, 44 responded and provided data on cases. In total, 107 patients were included, 106 of whom were male. The mean age of the patients was 19 years (range 5–40 years). The initial site, with more than one possible at the same time, was back of the head/occipital in 90 cases (84%), temporal/retroauricular in 17 cases (15.8%), facial in 4 (3.7%), periauricular in 2 (1.8%), back in 1 (1%), and not specified in 2 (1.8%) (Fig. 1a). In the majority of cases (65 [60.7%]), infection had not spread to other areas; when it had, the most affected areas are those shown in Fig. 1b.
 Initial site of lesions of tinea capitis recorded in the present study, marked with red dots. Note the predominance of areas that are shaved (back of the head and temporal area). (B) Spread to other sites in the present series, marked with blue dots.")
Inflammatory forms were reported in 29 patients (21.1%) compared with 78 (72.9%) that were not inflammatory. The most frequently reported causative agent in the series was T. tonsurans, with 81 confirmed cases (75.7%), followed by T. rubrum, T. mentagrophytes and T. verrucosum, M. canis, and M. audouinii (Table 1). Of the total 81 cases of ringworm caused by T. tonsurans, 22 (27.1%) were inflammatory. Of the total 29 cases of inflammatory ringworm, 21 (72.4%) were caused by T. tonsurans.
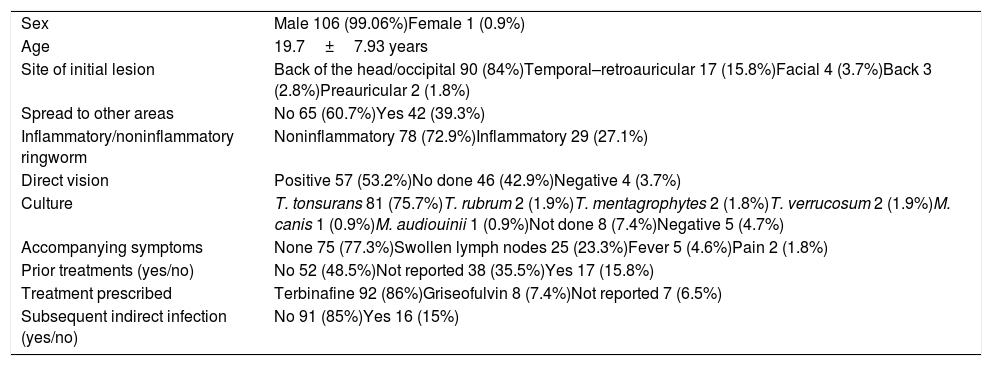
Results.
| Sex | Male 106 (99.06%)Female 1 (0.9%) |
| Age | 19.7±7.93 years |
| Site of initial lesion | Back of the head/occipital 90 (84%)Temporal–retroauricular 17 (15.8%)Facial 4 (3.7%)Back 3 (2.8%)Preauricular 2 (1.8%) |
| Spread to other areas | No 65 (60.7%)Yes 42 (39.3%) |
| Inflammatory/noninflammatory ringworm | Noninflammatory 78 (72.9%)Inflammatory 29 (27.1%) |
| Direct vision | Positive 57 (53.2%)No done 46 (42.9%)Negative 4 (3.7%) |
| Culture | T. tonsurans 81 (75.7%)T. rubrum 2 (1.9%)T. mentagrophytes 2 (1.8%)T. verrucosum 2 (1.9%)M. canis 1 (0.9%)M. audiouinii 1 (0.9%)Not done 8 (7.4%)Negative 5 (4.7%) |
| Accompanying symptoms | None 75 (77.3%)Swollen lymph nodes 25 (23.3%)Fever 5 (4.6%)Pain 2 (1.8%) |
| Prior treatments (yes/no) | No 52 (48.5%)Not reported 38 (35.5%)Yes 17 (15.8%) |
| Treatment prescribed | Terbinafine 92 (86%)Griseofulvin 8 (7.4%)Not reported 7 (6.5%) |
| Subsequent indirect infection (yes/no) | No 91 (85%)Yes 16 (15%) |
Culture was not done in 8 cases (7.4%), while 5 (47%) yielded a negative result. The most common accompanying clinical symptoms were swollen lymph nodes in 25 cases (23.3%), fever in 5 (4.6%), and pain 2 (1.8%). In 16 cases (15%), subsequent indirect contagion to family members or partners of the index cases was reported.
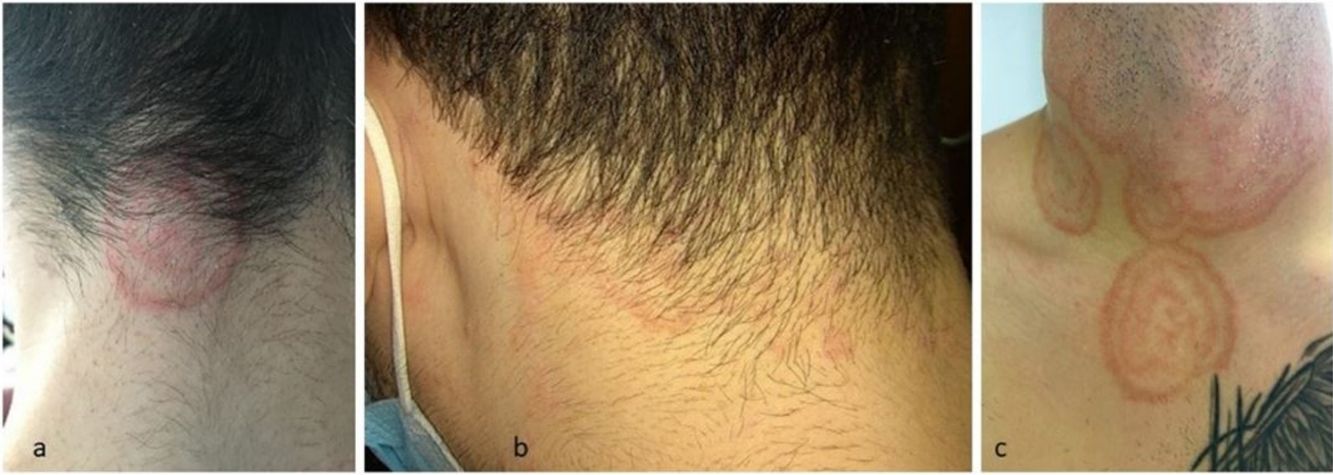
Figs. 2 and 3 show different images of the inflammatory and noninflammatory forms reported in the present study. Fig. 4 shows typical trichoscopic findings of black dots and corkscrew hair, indicative of noninflammatory forms. Fig. 5a shows typical trichophytic patterns on direct examination with KOH, and Fig. 5b an image of an isolate of T. tonsurans.
 Noninflammatory forms. (C) Spread to areas away from the initial site.")


 Parasitization in the KOH examination. (B) Septate hyphae and arthroconidia in the KOH examination. (C) Isolate of T. tonsurans in glycosylated Sabouraud agar with actidione.")
The most widely used treatment was oral terbinafine (250mg/d) in 92 cases (86%), with a median duration of 2 months (range 1–3 months). Griseofulvin was used in 8 patients (7.4%) and 23 patients (21.4%) also received topical treatment in addition to systemic treatment. Response to treatment was favorable, with complete cure in all cases without any reports of relapse.
Fifty-two patients had not received any prior treatment; 17 (15.8%) had applied topical corticosteroids, either on their own initiative or following prescription by the primary care physician, 16 (15%) applied topical antifungal agents, and 5 (5.6%) took systemic antibiotics. There was a relationship between inflammatory forms and previous corticosteroids use.
DiscussionThe present study is the most extensive one of cases of ringworm of the scalp associated with a visit to the hairdressers published to date. The design was retrospective and with a limited number of participating dermatologists. Its objective was not to obtain an estimate of the total number of cases in Spain nor the geographic distribution but rather provide a sufficiently representative sample of cases to define the clinical pattern, etiology, and response to treatment. The outbreak affects almost exclusively young males who frequently shave the back of the head and temporal area in hairdressers, often every week or twice a month, generally on Fridays, to prepare for going out on the weekend. This fashion seems to be a response to the haircuts of certain footballers, Tiktokers, or DJs.11
The observation that supports this practice as the cause of the outbreak is the area of the body where the initial lesion appears, which coincides with the most closely shaved hair, and therefore, the greatest contact between the razor and skin. We observed a frequent delay in diagnosis, as well as application of ineffective treatments, including topical corticosteroids, which may lead to rapid dissemination of fungal infection to other areas.
The most frequently isolated agent was T. tonsurans, in line with the increasing incidence of this dermatophyte infection in Europe.7 The cause of the increase in prevalence of ringworm of the scalp due to T. tonsurans has not yet been determined. One reason could be that griseofulvin, the only systemic antimycotic agent approved in children, is not as effective as terbinafine in the treatment of trichophyton infection, such as that caused by T. tonsurans. As a result, inappropriate therapy could lead to spread of infection. Only around half of all mycoses caused by T. tonsurans have been successfully treated by applying griseofluvin, as terbinafine would be the treatment of choice. In those caused by T. tonsurans and T. schoenleinii, much longer courses of treatment may be needed and, at times, with full doses (20mg/kg/d) of griseofulvin.1
Although noninflammatory ringworm predominates, as expected when T. tonsurans is the causative agent, more than one fourth of ringworm infections caused by T. tonsurans in our series were inflammatory, a significant number and in line with that reported for the German outbreak.7 One possible explanation would that microtraumas during shaving could be associated with more extensive invasion, and therefore, a greater host immune response.
Detailed medical history usually provides important information on the possible origin of the disease in those outbreaks transmitted by contaminated hairdressing utensils. To interrupt the chain of infection, mycological study is urgently indicated for contacts of the index case, as well as antimycotic therapy for asymptomatic carriers of the fungus, who would need to be identified by microbiological tests. In addition, appropriate and constant hygiene measures should be taken with the hairdressing utensils of common use in accordance with the current guidelines that indicate that parts in contact with the skin should be disposable or sterilized in an autoclave.12 Spores from dermatophytes can persist on inanimate objects (including brushes, towels, cushions, and electric razors). There have even been reports of asymptomatic carriers who have spores in the scalp and who do not develop the disease, but they can transmit the pathogen. In fact, T. tonsurans is the dermatophyte species associated with asymptomatic carriers.13
In conclusion, the present study describes an emerging epidemiologic situation for which a deeper understanding is necessary with future studies that include information on patients and their contacts, hairdressers, and their hygiene habits, as well as field studies with mycological cultures of material from shaving, and other pertinent actions, in particular, public health education. The high number of cases supposedly transmitted by hairdressing utensils should be taken into account by the corresponding public health bodies, who need to ensure compliance with the established guidelines for disinfection.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Vicent Alonso, Salomé Álvarez, Asunción Arregui, Belén Civico, Víctor Dios, Patricia Eguino, Andrea Estébanez, Vicente Expósito, Santiago Férnández de Piérola, Patricia Garbayo, Elisabeth Gómez, M. Rosario González-Hermosa, José Herrerías, Helena Iznardo, Ane Jaka, Mar Llamas, Irene López, Miren Marquina, Júlia Mercader, Joan F. Mir, Juan A. Moreno, Juan M. Morón, Carolina Ortuño, Nasser Porras, Liliana Randazzo, Amparo Sánchez, Júlia Sánchez-Schmidt, Jesús Tercedor, Tomás Toledo, Anna Tuneu, Pedro Vilas, Susana Vildósola, Jorge Adsuar.


