

Primary cutaneous CD8+ T-cell lymphoma has been included as a provisional entity within the new revised classification of lymphoid neoplasms of the World Health Organization in 20161. It was initially described as indolent CD8+ lymphoid proliferation of the ear2 and a total of 29 cases of such neoplasm have been published in the literature so far. None of them have been linked to delayed contact hypersensitivity reactions. We present a case of acral type primary cutaneous lymphoma T CD8+ involving both earlobes clearly related with the prolonged use of gold earrings, confirmed with epicutaneous tests, histopathology, immunohistochemical and molecular studies. Auricular skin lesions were induced again with a provocation test with identical histopathologycal and the same clonality, confirming both the diagnosis of lymphoma and its induction by the antigenic stimulus of gold.
El linfoma cutáneo primario T CD8+ tipo acral ha sido incluido como entidad provisional dentro de la nueva clasificación revisada de las neoplasias linfoides de la Organización Mundial de la Salud en 20161. Inicialmente fue descrito como proliferación linfoide CD8+ indolente de la oreja2, y se han publicado en la literatura un total de 29 casos de dicha neoplasia. Ninguno de ellos se ha relacionado con reacciones de hipersensibilidad retardada de contacto. Presentamos un caso de linfoma cutáneo primario T CD8+ tipo acral auricular bilobular en clara relación etiológica con el uso prolongado de unos pendientes de oro confirmada con pruebas epicutáneas, estudio histológico, inmunohistoquímico y molecular. Las lesiones cutáneas bilobulares fueron inducidas de nuevo con un test de uso e idénticos resultados a los iniciales y misma clonalidad, lo cual terminó de confirmar tanto el diagnóstico del linfoma como su inducción por el estímulo antigénico del oro.
Gold is a very stable metal in the epidermis and rarely causes allergic contact eczemas. However, when present in the dermis, it can form ions and remain for long durations and so has been associated with pseudolymphomatous allergic contact dermatitis caused by gold earrings. Persistent antigenic stimulus by gold is the cause we propose in the case we describe below, with the particular and exceptional circumstance that this is a true primary cutaneous lymphoma and not a pseudolymphomatous lymphomatoid contact dermatitis. This is the first report in the literature of indolent primary cutaneous acral CD8+ T-cell lymphoma induced by gold earrings.
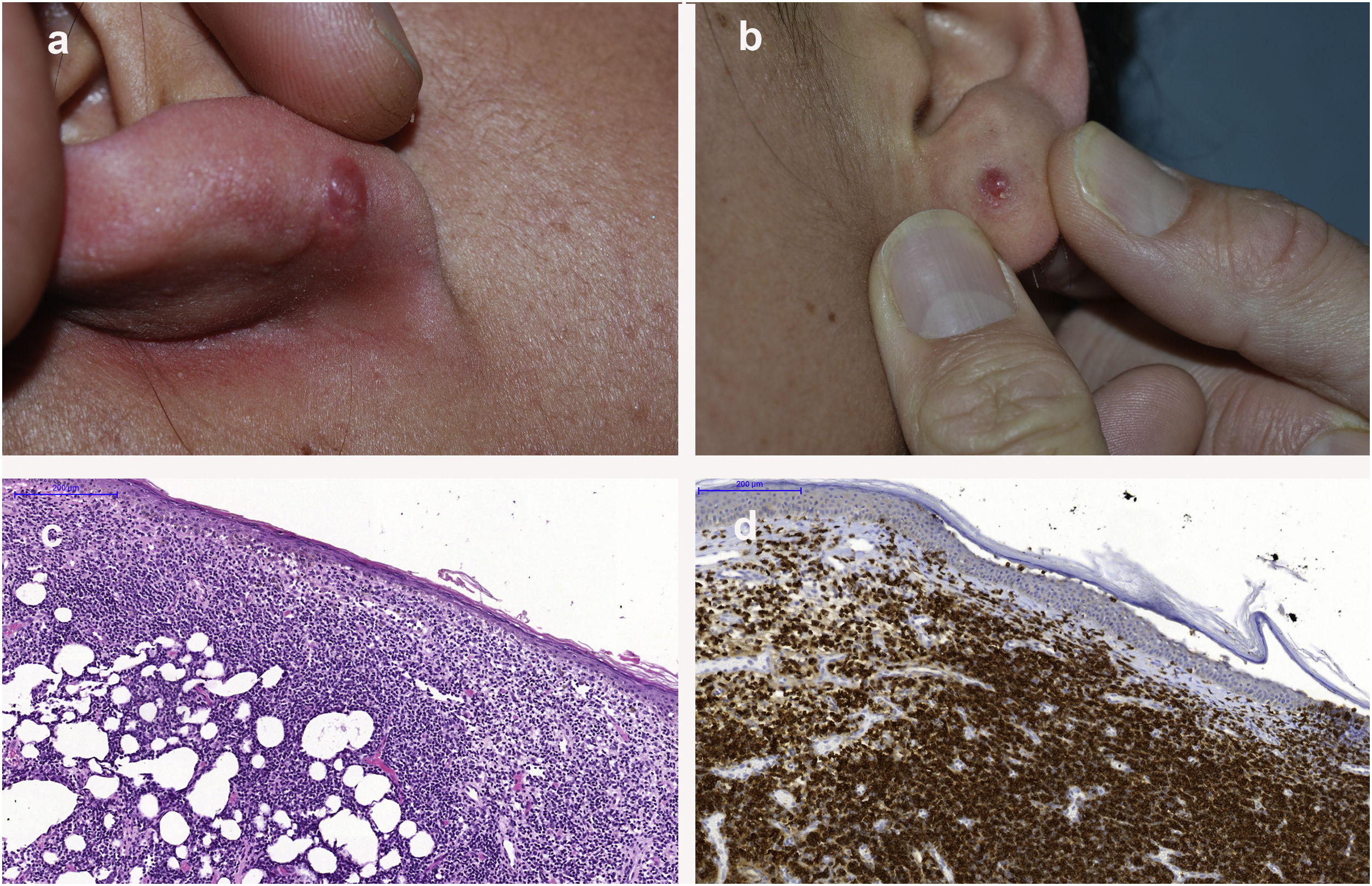
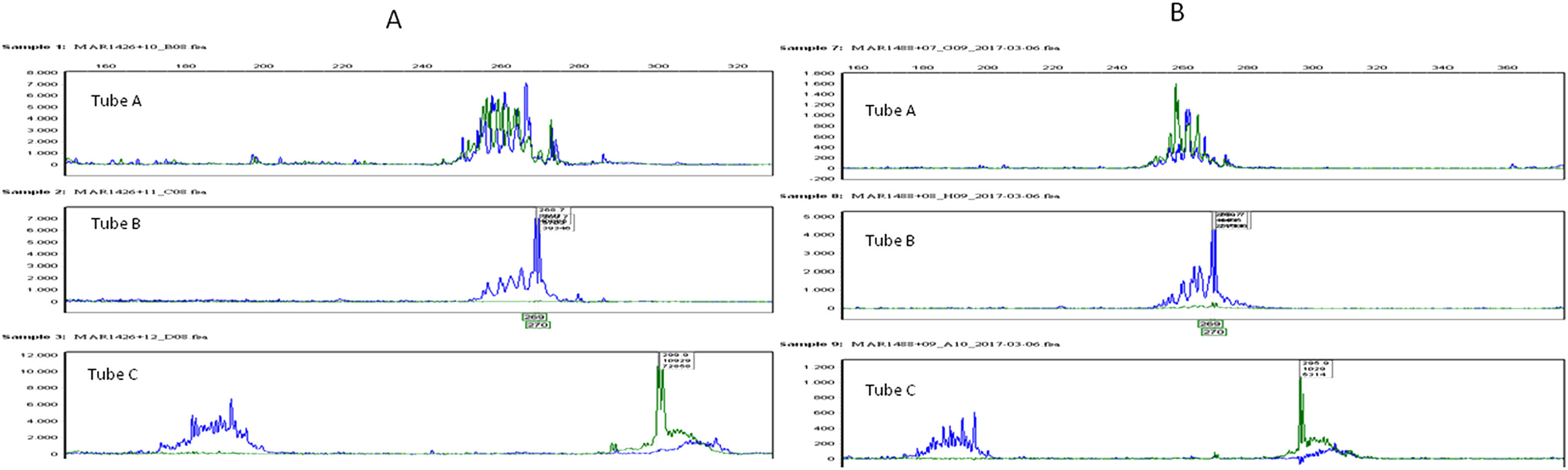
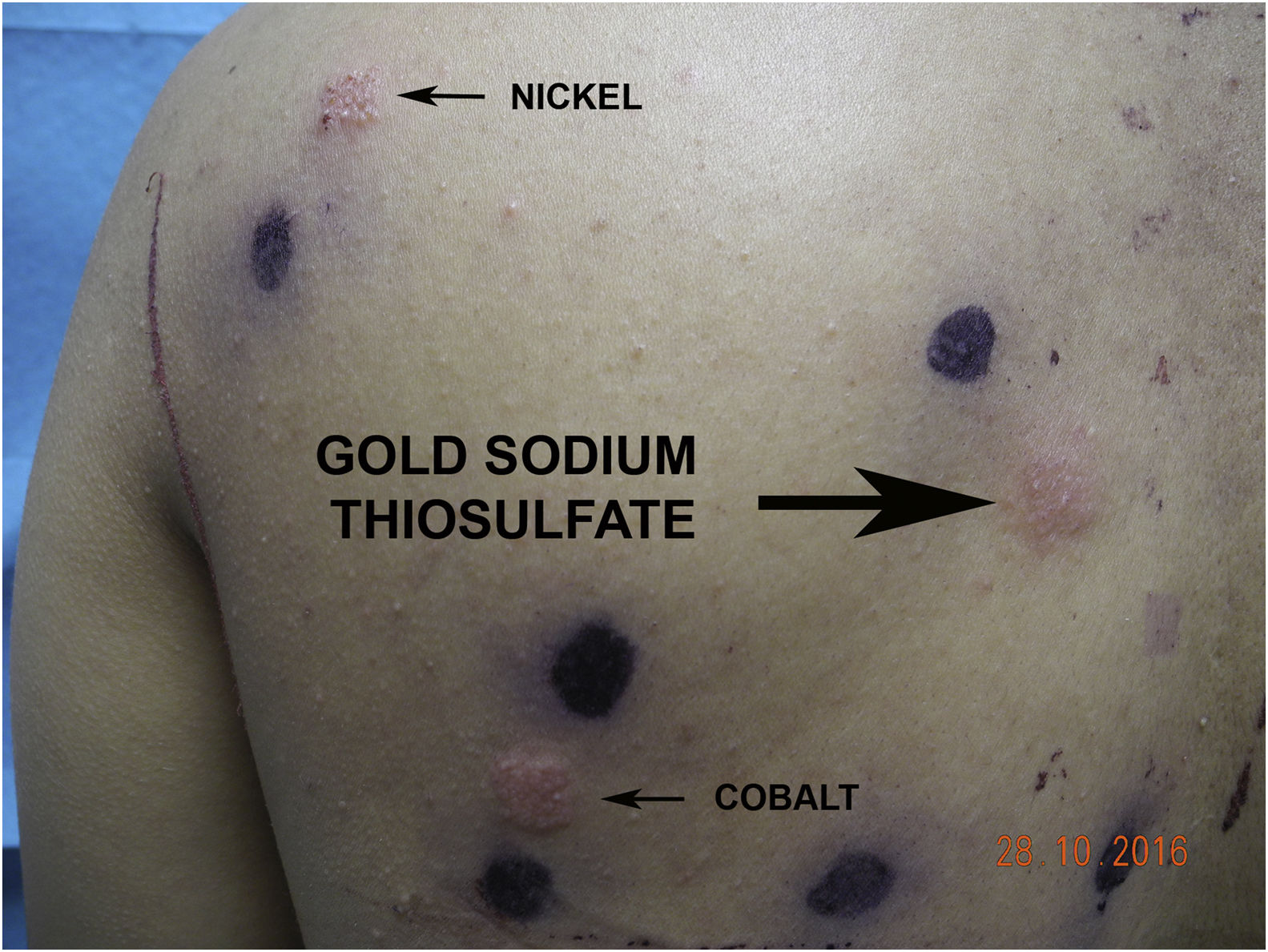
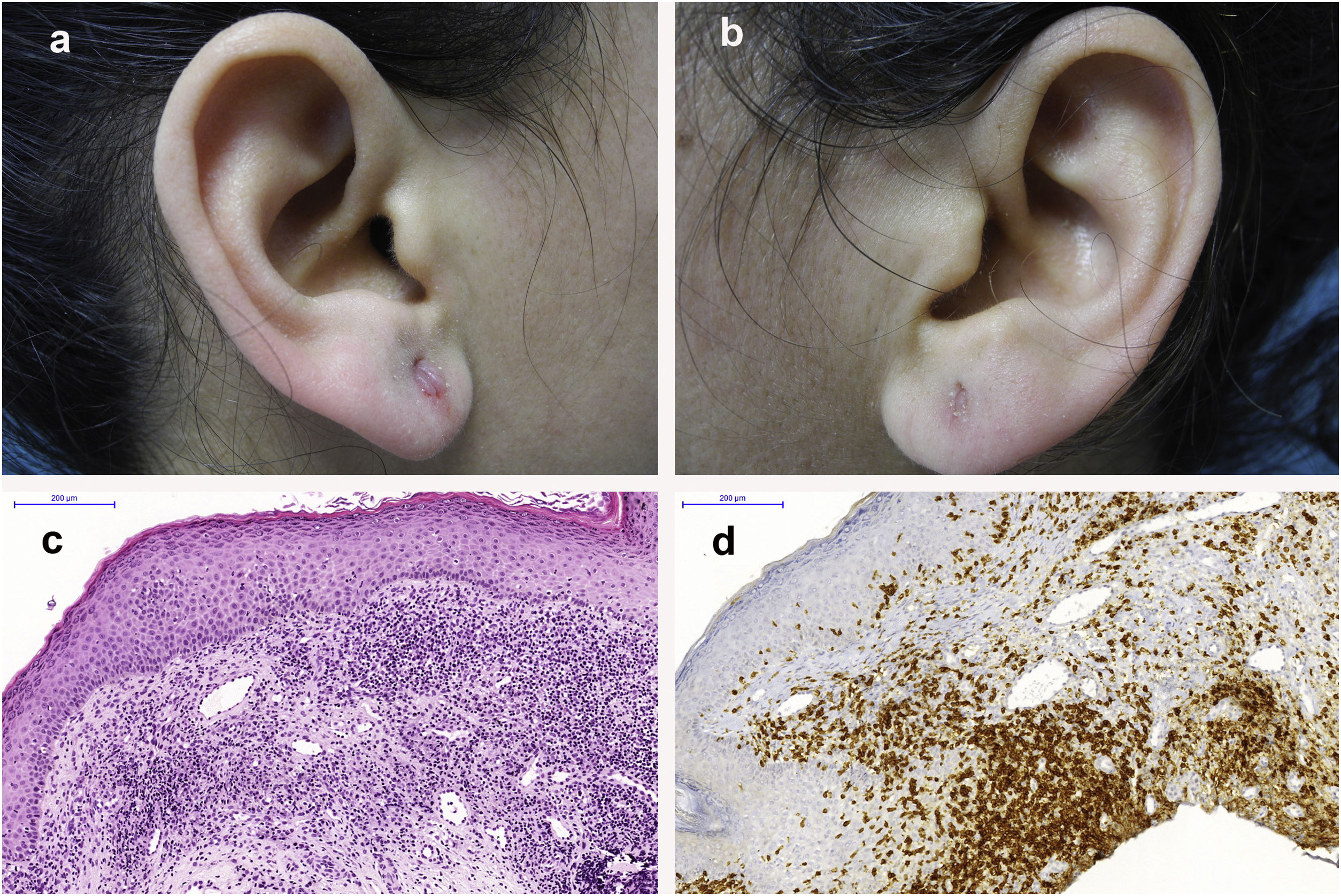
Case HistoryA 30-year-old woman, with no clinical history of interest except intolerance of jewelry, attended the clinic because of persistent papular lesions in both ear lobes. The lesions had appeared 1 year earlier. Growth had been slow and the lesions were located on the internal face of both lobes (the left-sided lesion had spread to the external face) at the site of the earring hole. These lesions were reddish and indurated to touch, measuring 8 and 10 mm in diameter (Fig. 1A and B). The patient reported using only 2 pairs of gold earrings in the previous 6 years. Within a few hours, these caused pruritus, erythema, and scaling which resolved after removing them. Nevertheless, she continued to use them until the bilateral papular lesions in the earlobes appeared. Given the clinical suspicion of cutaneous pseudolymphoma or lymphomatoid contact dermatitis due to persistent antigenic stimulus by gold, we performed an excision biopsy of both earlobe lesions, as well as patch tests. The histopathological findings for both lesions were the same. A dense and diffuse lymphoid infiltrate was observed occupying the entire dermis but sparing the epidermis and skin appendages. This infiltrate was formed of atypical small and medium-sized CD8+ T lymphocytes with no necrosis or angiodestructive changes and with limited epidermotropism (Fig. 1C and D). There was no evidence of lymphoid follicles with reactive germinal centers. Immunohistochemical study identified T lymphocytes positive for CD2, CD3, CD5, and CD7, with a clear predominance for CD8. TIA 1 and ß-F1 markers were positive whereas CD4, CD20, CD30, CD56, granzyme B, and EBERS were negative and Ki-67 positivity was weak (<5%). Study of T-cell receptor beta gene rearrangement showed monoclonal expansion in both lesions with the same clone (Fig. 2A), and primary cutaneous acral CD8+ T-cell lymphoma of both ear lobes was diagnosed. Study of extension, including positron-electron tomography/computed tomography, ruled out systemic extracutaneous spread. We also performed patch testing with the standard Spanish GEIDAC patch test series, applying the T.R.U.E Test® panel and supplementary allergens. The readout showed intense eczematous-vesicular positivity to gold sodium thiosulfate 1% and weaker positivity to nickel and cobalt (Fig. 3). The dimethylglyoxime test on both gold earrings was negative, ruling out the presence of nickel. Skin biopsy of the patch positive to gold sodium thiosulfate showed a dense reactive lymphohistiocytic infiltrate in the upper half of the dermis. The positive reactions to nickel and cobalt were considered of past relevance, whereas the reactions to gold represented current relevance as the inducer of the aforementioned cutaneous lymphoma through intermittent antigenic stimulus over the course of 6 years. To confirm this possible association, 6 months later, and without any evidence of recurrence of the lesions, we decided to perform a test of continuous use of the gold earrings to observe whether new papular lesions similar to those biopsied might appear. This was indeed the case. Five weeks after daily use, papular-erythematous lesions very similar to the previous ones reappeared in both earlobes at the earring hole (Fig. 4A and B). An excision biopsy was performed once more with the same findings as the previous one both in histopathological and immunohistochemical terms (Fig. 4C and D). TCR-beta molecular analysis also showed monoclonality, with the same clone as the initial lesions (Fig. 2B). The use test and its result confirmed that gold had been able to cause the primary cutaneous acral CD8+ T-cell lymphoma in both earlobes. In the 6 months after the use test, no relapses were observed as the patient stopped using the gold earrings.

 and those induced by the use test (B). Note the identical monoclonal peak in both tubes B and C in the different samples.")
.")
. C and D, Identical findings in the biopsy of these lesions with hematoxylin and eosin staining and immunohistochemical study ×100 as in Fig. 1C and D (initial lesions).")
A and B, Papular lesions at the same site 5 weeks after rechallenge with the gold earrings (use test). C and D, Identical findings in the biopsy of these lesions with hematoxylin and eosin staining and immunohistochemical study ×100 as in Fig. 1C and D (initial lesions).
Primary cutaneous acral CD8+ T-cell lymphoma has been included as a provisional entity in the new revised classification of lymphoid neoplasms published by the World Health Organization in 2016,1 along with indolent T-cell lymphoproliferative disease of the gastrointestinal tract. Both entities are clonal disorders composed of cytotoxic CD8+ T lymphocytes and an indolent clinical course.1
The cutaneous entity was originally described by Petrella et al.2 in 2007 under the denomination indolent CD8+ lymphoid proliferation of the ear, given its course and favorable prognosis. Subsequent publications extended the clinical, histopathological, and immunohistochemical description of this neoplasm and reported features differentiating it from other primary cutaneous cytotoxic T-cell lymphomas.3,4 Cutaneous lesions in form of erythematous papules and nodules have not just been described on the ear but also the face3,5 (nose, lower eyelid) and feet and hands,6 and so the term acral was added as a generic description of the site.6 According to Li et al.4 the acral predilection of the lesions (although they predominate on the ear and face4) may suggest an as yet to be determined specific immune stimulus, which in none of the 29 cases published to date4,6,7 has been associated with phenomena of type IV delayed hypersensitivity. Most cases show very characteristic histopathological, immunohistochemical, and molecular characteristics. An atypical dense and diffuse monomorphic lymphocyte infiltrate is usually observed, occupying the dermis with limited epidermotropism and no reactive lymphoid follicles. In no case has any necrosis or destruction of appendages and vessels been observed. The proliferative index is usually low, except in the 3 cases described by Greenblatt et al.,6 although the clinical course was also indolent. Systemic extracutaneous involvement has not been reported except in a single case.8 Recurrences have not been reported in almost all patients after excission or local radiotherapy, except in 5 who did not return after a second treatment.4,6 The median duration of follow-up was 2 years.6 Immunohistochemistry revealed positivity and predominance of CD8+ lymphocytes and a cytotoxic α/ß (ß-F1+) T-cell phenotype, and negativity for CD56, CD30, and granzyme B. Gene rearrangement study of the TCR gene showed monoclonality in 20 cases and negativity in 4, while no result was available in 5.4,6,7
In the literature, there are little more than 10 cases of rare pseudolymphomatoid allergic contact dermatitis caused by gold earrings,9–18 but in all cases, histopathology points to cutaneous pseudolymphoma and not true lymphoma. The main difference lies in the mixed character of the dermal cellular infiltrates and the presence of reactive lymphoid follicles.12,13,18 In almost all cases, the characteristic CD8+ phenotype and clonality studies are lacking. Recently, Kiyohara et al.19 have reported a case of papular pseudolymphoma induced by a gold patch test and Rodríguez-Villa Lario et al.20 reported a case of pseudolymphoma B of the upper eyelid associated with a gold weight implant.
Its etiopathogenesis appears to involve persistent antigenic exposure to gold located in the dermis, as the metal has a greater tendency to ionize in this location than in the epidermis,18 where it is usually much more stable. For the gold to be antigenic and induce a delayed type IV hypersensitivity reaction, it had to be converted to a small soluble form through the effect of amino acids from sweat and be absorbed. Once in the dermis, this soluble form can remain for a long time in the extracellular fluid or matrix and thus represent a sustained immune stimulus21 able to induce pseudolymphomatous lymphomatoid allergic contact dermatitis9–13,17,18 or indeed lymphoma, as in our case. Given that the CD8+ lymphocytes are involved in triggering the innate immune response to haptens, one hypotheses that connects both entities is that a continual and lasting allergenic stimulus could induce clonal lymphoproliferative disease in a susceptible host instead of a reactive lymphocyte reaction. This capacity to remain in soluble form in the dermis could thus explain the frequently observed and well-known persistent positive results to gold sodium thiosulfate.
This is the first report in the literature of indolent primary cutaneous acral CD8+ T-cell lymphoma induced by gold earrings. The causative agent was confirmed by the use test that once again reproduced the lesions with the same histological, immunohistochemical, and molecular findings as in the initial lesions. The presence of the same clone in 2 different lesions (the initial ones) and at different time points (those induced by the use test) is very suggestive of lymphoma.
In none of the 29 reported cases of this lymphoma has onset been attributed to any contact allergen or to gold earrings, even though the most frequent site is the ear (17 out of 29 cases, 59%), with the helix being more often involved then the earlobe. Likewise, we have not found any cases published in the literature of true primary cutaneous lymphomas or systemic lymphomas related to sustained contact allergenic induction.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Molinero Caturla J, Sánchez Sánchez J, Marcoval Caus J, Muniesa Montserrat C, Climent Esteller J, Servitje Bedate O. Linfoma cutáneo primario T CD8+ tipo acral inducido por hipersensibilidad retardada persistente a pendientes de oro. Actas Dermosifiliogr. 2021;112:649–653.



