




The first reported cases of allergic contact dermatitis from acrylates in manicure procedures in relation to the application of porcelain nails were published decades ago. The frequency of sensitization has increased due to the introduction of the so-called permanent nail polish containing photo-bonded acrylates, mainly involving the beauticians who apply them, and to a lesser extent, the consumers. The recent commercialized permanent polish kits for domestic use could trigger even higher degrees of sensitization. In this article, the clinical features, diagnostic procedures, treatment and preventive measures are described. Acrylates are present in a wide range of sources including multiple medical materials. Sensitization caused by a merely aesthetic procedure might end up having an eventual important impact in the future consumer's health which is why restrictive policies should be implemented limiting its use to qualified professionals and banning the indiscriminate sale of domestic kits.
Los primeros casos de dermatitis alérgica de contacto por acrilatos en procedimientos de manicura se describieron hace décadas en relación con la aplicación de uñas de porcelana. Recientemente se ha incrementado la frecuencia de sensibilización secundariamente a la implantación de los llamados esmaltes permanentes que contienen acrilatos UV curables, predominantemente entre las esteticistas que los aplican y en menor medida en usuarias. La reciente comercialización de kits de uso doméstico podría precipitar un aumento en la frecuencia aún mayor. En este artículo describimos su técnica de aplicación, la clínica, el diagnóstico, el tratamiento y la prevención. Los acrilatos están presentes en una amplia variedad de fuentes, incluidos múltiples materiales médicos. Una sensibilización desencadenada por un procedimiento puramente estético podría llegar a tener una importante repercusión en la salud, por lo que se imponen políticas restrictivas por parte de las autoridades que limiten su uso a profesionales cualificados y prohíban la venta indiscriminada de kits caseros.
Acrylates and methacrylates are plastic materials formed by the polymerization (curing) of monomers derived from acrylic acid or methacrylic acid. Acrylic monomers are responsible for most acrylate-induced allergic contact dermatitis (ACD) reactions. On completion of the curing process, acrylic compounds become relatively inert—because of their high molecular weight—and therefore cease to have sensitizing properties. However, the persistence of monomers under deficient polymerization conditions can induce sensitization or cause a contact dermatitis reaction in a previously sensitized individual.1
Acrylic polymers have numerous uses, including the manufacture of electrical insulators, compact discs, paints, adhesives, and printing inks.2 Acrylates have also been used in the manufacture of various medical devices, including contact lenses, intraocular lenses, dental prostheses, composite fillings, bone cement, insulin pumps, and hearing aids. Polymethyl methacrylate is capable of absorbing several times its weight in water and is therefore used in the manufacture of disposable diapers and sanitary napkins,3,4 as well as certain types of bandages, ulcer dressings, and incontinence pads.5 The first cases of acrylate-induced ACD were reported in occupational contexts. The professionals at the greatest risk of exposure to acrylates include dentists, dental technicians, orthopedic surgeons, people who work in the printing or fiberglass industries, and individuals exposed to paints or adhesives.6
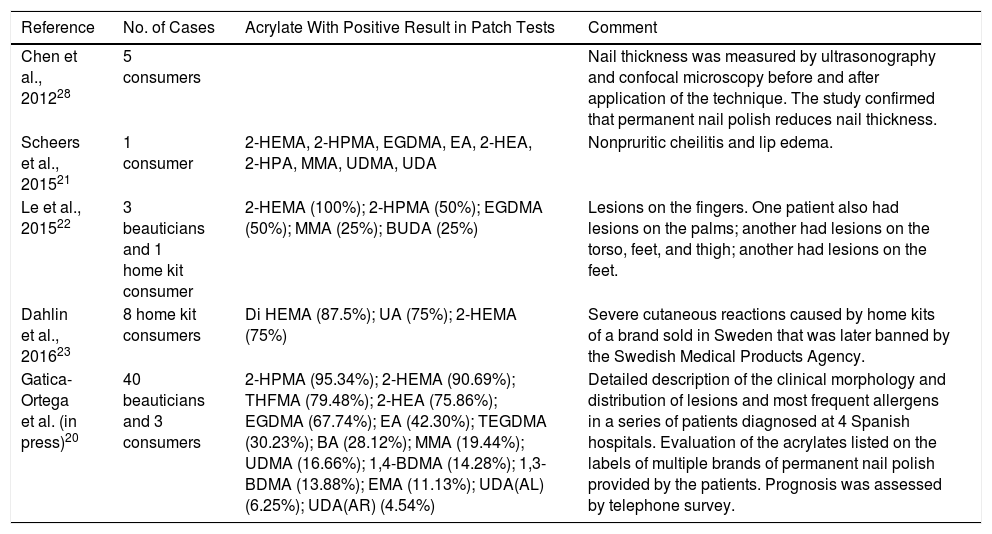
The first case of ACD caused by the acrylic materials used in artificial nails was reported in 1956.7 Since then, numerous cases of acrylate-induced ACD have been reported in association with the application of this technique for cosmetic reasons or for professional purposes, as in the case of a flamenco guitarist.8 Following the introduction of so-called “gel nails,” an increase in the frequency of sensitization was observed.9–13 Permanent nail polish—also known as long-lasting nail polish or semipermanent nail polish—is a new type of polish containing acrylates that first appeared on the market around the year 2010. In recent years, the frequency of acrylate-induced ACD has increased considerably, especially in patients sensitized by this new manicure technique, which is currently the leading cause—by a wide margin—of acrylate sensitization in Spain. Nevertheless, few studies have been published on this subject (Table 1). It is likely that many of the cases of ACD secondary to “gel nails” that have been reported in recent years were actually caused by permanent nail polish. Since both procedures involve the use of UV light to initiate the curing process, it is possible that in some cases the patient or physician was unable to specify exactly which of the two procedures was used if the medical history was not very specific.
Review of the Literature on Permanent Nail Polish.
| Reference | No. of Cases | Acrylate With Positive Result in Patch Tests | Comment |
|---|---|---|---|
| Chen et al., 201228 | 5 consumers | Nail thickness was measured by ultrasonography and confocal microscopy before and after application of the technique. The study confirmed that permanent nail polish reduces nail thickness. | |
| Scheers et al., 201521 | 1 consumer | 2-HEMA, 2-HPMA, EGDMA, EA, 2-HEA, 2-HPA, MMA, UDMA, UDA | Nonpruritic cheilitis and lip edema. |
| Le et al., 201522 | 3 beauticians and 1 home kit consumer | 2-HEMA (100%); 2-HPMA (50%); EGDMA (50%); MMA (25%); BUDA (25%) | Lesions on the fingers. One patient also had lesions on the palms; another had lesions on the torso, feet, and thigh; another had lesions on the feet. |
| Dahlin et al., 201623 | 8 home kit consumers | Di HEMA (87.5%); UA (75%); 2-HEMA (75%) | Severe cutaneous reactions caused by home kits of a brand sold in Sweden that was later banned by the Swedish Medical Products Agency. |
| Gatica-Ortega et al. (in press)20 | 40 beauticians and 3 consumers | 2-HPMA (95.34%); 2-HEMA (90.69%); THFMA (79.48%); 2-HEA (75.86%); EGDMA (67.74%); EA (42.30%); TEGDMA (30.23%); BA (28.12%); MMA (19.44%); UDMA (16.66%); 1,4-BDMA (14.28%); 1,3-BDMA (13.88%); EMA (11.13%); UDA(AL) (6.25%); UDA(AR) (4.54%) | Detailed description of the clinical morphology and distribution of lesions and most frequent allergens in a series of patients diagnosed at 4 Spanish hospitals. Evaluation of the acrylates listed on the labels of multiple brands of permanent nail polish provided by the patients. Prognosis was assessed by telephone survey. |
Abbreviations: BA, butyl acrylate; 1,4-BDMA, 1,4-butanediol dimethacrylate; 1,3-BDMA, 1,3-butanediol dimethacrylate; BUDA, butanediol diacrylate; Di HEMA, Di-HEMA trimethylhexyl dicarbamate; EA, ethyl acrylate; EGDMA, ethylene glycol dimethacrylate; EMA, ethyl methacrylate; 2-HEA, 2-hydroxyethyl acrylate; 2-HEMA, 2-hydroxyethyl methacrylate; 2-HPA, 2-hydroxypropyl acrylate; 2-HPMA, 2-hydroxypropyl methacrylate; MMA, methyl methacrylate; TEGDMA, triethylene glycol dimethacrylate; THFMA, tetrahydrofurfuryl methacrylate; UA, urethane acrylate; UDA, urethane diacrylate; UDA(AL), aliphatic urethane dimethacrylate; UDA(AR), aromatic urethane dimethacrylate; UDMA, urethane dimethacrylate.
In this article, we describe acrylate-induced ACD associated with various nail-care procedures, with special emphasis on ACD secondary to the use of permanent nail polish, which is currently very popular. Specifically, we describe the application technique, clinical presentation, diagnosis, treatment, and prevention measures.
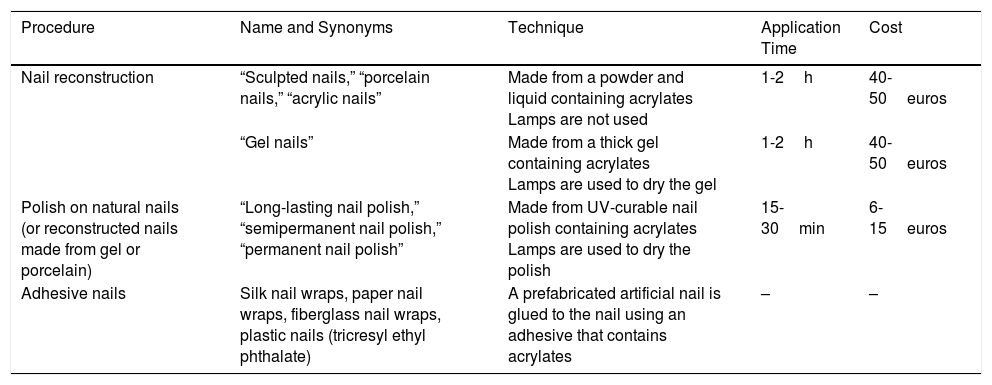
Long-Lasting Nail Polish: Application TechniqueThere are 4 types of manicure techniques that involve the use of acrylic materials (Table 2). In this section, we provide further details about the new permanent nail polish technique.
Main Characteristics of Manicure Techniques Involving Acrylates.
| Procedure | Name and Synonyms | Technique | Application Time | Cost |
|---|---|---|---|---|
| Nail reconstruction | “Sculpted nails,” “porcelain nails,” “acrylic nails” | Made from a powder and liquid containing acrylates Lamps are not used | 1-2h | 40-50euros |
| “Gel nails” | Made from a thick gel containing acrylates Lamps are used to dry the gel | 1-2h | 40-50euros | |
| Polish on natural nails (or reconstructed nails made from gel or porcelain) | “Long-lasting nail polish,” “semipermanent nail polish,” “permanent nail polish” | Made from UV-curable nail polish containing acrylates Lamps are used to dry the polish | 15-30min | 6-15euros |
| Adhesive nails | Silk nail wraps, paper nail wraps, fiberglass nail wraps, plastic nails (tricresyl ethyl phthalate) | A prefabricated artificial nail is glued to the nail using an adhesive that contains acrylates | – | – |
Proper application of permanent nail polish involves several steps. The first step is to prepare the nail by removing any traces of previously applied nail polish. Then the upper surface of the nail and the exposed portion of the lower surface are thoroughly scrubbed using a clean, disinfected brush with soft bristles. A fine-grain (180-240 grit) file is then used to smooth the surface of the nail and isopropyl alcohol—which has a drying effect—is applied in order to remove any residual moisture or oil.14,15 Then, as in the application of conventional nail polish, a soft brush is used to apply 3 or more consecutive coats of polish. The base coat and top coat are transparent; the intermediate coat(s) contain the pigments responsible for the final color. All of these coats of polish contain acrylates that polymerize on exposure to a light source in the presence of photoinitiators. During the curing process, the polish becomes hard and dry. The pigments used in the intermediate coat(s) are the same as those in conventional nail polish. Some beauticians use 2 curing lamps—1 on either side of the manicure station—while others use just 1 lamp at the center of the table. If there is only 1 lamp, the customer places a hand under the lamp for curing while the beautician paints the nails on the other hand (Fig. 1). The light source can be a low-intensity UV-A lamp, generally with a wavelength in the range of 325-435nm. Under this sort of lamp, the polish dries in approximately 2minutes. Some beauticians have started to use light-emitting diode (LED) lamps, which reduce the drying time to approximately 30seconds. The light bulbs must be changed every 2-4 months (depending on frequency of use) in order to guarantee the complete polymerization of the acrylic molecules.16 The final step is to once again clean the nails with isopropyl alcohol. In some cases, essential oils are also applied at the end of the procedure. A trained beautician can complete the entire permanent nail polish technique in just 15-30minutes.
. Note that the thumb of the left hand is not under the lamp. In order for acrylate to polymerize properly, the thumb must later be placed under the light separately.")
Permanent nail polish stays shiny and intact for approximately 3-4weeks, although a strip of unpolished nail eventually becomes visible as the nails grow. The polish must then be removed and reapplied. In this regard, the permanent nail polish procedure is different from that of acrylic nails, which are not removed entirely but instead undergo a maintenance process called “rebalancing” in which the strip of bare nail is filled in.
To remove the polish, the customer's fingers are submerged in a recipient filled with solvent (usually acetone) for at least 15-20minutes. An alternative method is to douse cotton balls in solvent and hold them in place on the nails using special clips or aluminum foil. In some cases, a nail drill must be used to remove the polish completely.
The nail care field is booming and innovative variants are constantly being introduced. The 2 most important innovations in permanent nail polish are as follows:
- 1.
“Magnetic” or “3D effect” nail polish: Polishes containing metallic particles are sold with a magnet that is used to create a pattern. After the polish has been applied, the magnet is held very close to the nail. The metallic particles rise up towards the magnet, creating a gradient pattern that produces a luminous 3-dimensional effect. The polish is then dried under the lamp. The metals used in most magnetic nail polishes—iron(II,III) oxide (Fe3O4) or other alloys—have good magnetic and cosmetic properties and low sensitizing capacity. However, there has been a report of a case of ACD caused by magnetic nail polish that contained nickel and cobalt but was not labeled accordingly.17
- 2.
Digital nail art: A printer designed specifically for nail art is used to print images on natural or artificial nails. When this technique is used on natural nails, a base coat of polish is applied, followed by a coat of white polish that absorbs the ink. The next step is to print the desired image—a predesigned drawing or photograph—onto the nail. Finally, a top coat is applied. With natural nails, this technique can only be applied to one nail at a time; with artificial nails, it is possible to print on multiple nails (up to 20) at the same time. The printer is equipped with a screen that allows the beautician to adjust the image to the size of the nail. It also has a camera and a USB port.
Both of these innovations can be used with either conventional or permanent nail polish.
Allergic Contact Dermatitis Induced by Permanent Nail PolishClinical ManifestationsDifferent clinical forms of ACD are found in beauticians and consumers. In beauticians, ACD lesions caused by acrylates in permanent nail polish have a characteristic distribution and each site has an explanation. The lesions often appear on the finger pads, especially on the first fingers of the dominant hand. In the acute phase, when symptoms first appear, the lesions are exudative and pruritic, later progressing to a dry, fissured chronic pulpitis with subungual hyperkeratosis, with pain as the predominant symptom. Lesions on the hands are caused by direct contact with nail polish (Fig. 2). Many beauticians use their dominant hand—the one they use to hold the brush—to remove excess polish before the UV curing process, rather than using an orange wood cuticle stick for this purpose. In half of cases, eczematous lesions are seen at other sites besides the fingers, such as the dorsum of the nondominant hand, which some beauticians use to wipe off the finger used to remove excess polish (Fig. 3). The next most common site is the face, particularly the eyelids, cheeks, and jawline. Lesions at these sites are caused by passive transfer mechanisms (the fingers), contaminated objects such as mobile telephones, or, less frequently, airborne mechanisms. The airborne transfer mechanism appears to be less common in association with permanent nail polish than with acrylic nails because permanent nail polish does not involve any powdered components and the nails are filed before the polish is applied, so powder containing acrylates does not spread through the air. The neck can also be affected by the same mechanisms that cause lesions to appear on the face. Lesions on the area of the forearms that rests on the contaminated work table are also common. Lesions caused by accidental spillage of polish are also seen on the thighs and abdomen. Patients also sometimes present mild paresthesia, which they describe as a tingling sensation and decreased sensitivity in the fingers. Nearly all affected beauticians present a certain degree of onycholysis, subungual hyperkeratosis, and splinter hemorrhages. There have been no reports of severe paresthesia18 or onychodystrophy,19 which do occur in ACD caused by acrylic nails (Fig. 4)



Less frequently, ACD caused by the acrylates in permanent nail polish can be accompanied by edema of the eyelids or lips20,21 and/or mild symptoms of upper respiratory tract involvement.
There are 2 types of consumers of permanent nail polish: those who have the polish applied at a beauty salon, and those who apply it themselves using home kits. In beauty salon customers, lesions are seen on the hands—predominantly around the nails and on the finger pads—and, less frequently, on the face (eyelids and lips) and neck. In “amateur beautician” consumers—those who use home kits—the lesions are more extensive and intense, affecting the hands as well as other sites.22,23
DiagnosisTo confirm the diagnosis, the patient must undergo patch testing with a battery of acrylates used in artificial nails. In beauticians, however, clinical suspicion usually points to the correct diagnosis because the patients themselves attribute their symptoms to contact with permanent nail polish. Another possibility is to test for a smaller number of acrylates, for example, hydroxypropyl methacrylate (HPMA), hydroxyethyl methacrylate (HEMA), and tetrahydrofurfuryl methacrylate (THFMA). These acrylates are frequently present in permanent nail polish and are responsible for most reactions associated with these products. Because acrylates can evaporate, it is important to remember that they should be placed in the test chambers immediately before the patches are applied to the patient's back. Placing the acrylates in the chambers ahead of time and storing them at room temperature can result in false negatives.24 Patch tests tend to yield multiple positive results with intense (2+) or severe (3+) reactions and can cause “angry back” reactions and acquired leucoderma.18 Because of the risk of active sensitization and toxicity, it is not advisable to apply the products themselves directly. With these allergens, it is important to perform a delayed reading.
Unlike beauticians, consumers of permanent nail polish do not always associate their symptoms with exposure to these products. When a patient presents with eczema around the nails, on the face, or at any other site, the dermatologist must remember to consider this possibility and determine whether a temporal relationship exists. Clinical suspicion must be confirmed by patch testing with the same allergens recommended for beauticians.
TreatmentACD induced by exposure to permanent nail polish is treated in the same manner as other cases of ACD. Patients tend to respond to treatment with corticosteroids—topical or oral, depending on the severity of the symptoms—and, as in all cases of contact sensitization, the patient should be instructed to avoid the allergen as explained below.
Primary Prevention StrategiesMost beauticians are not adequately trained to prevent sensitization because they are unfamiliar with the risk posed by acrylates. Therefore, they handle permanent nail polish as they would conventional nail polish: without gloves, in direct contact with their bare hands, and without using appropriate materials such as orange wood cuticle sticks. Primary prevention strategies should target professional beauticians. As in any other industry where acrylates are handled, beauticians should receive adequate training on the risks involved in this type of work (Table 3). This training would also indirectly protect consumers of permanent nail polish. Nevertheless, consumers should also be informed about the risks associated with these products.
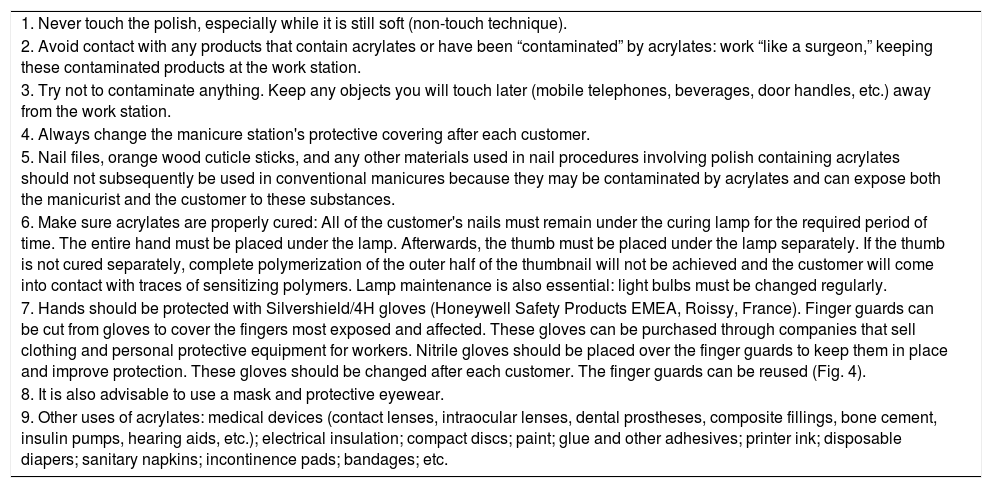
Recommendations for Beauticians Not Sensitized (Primary Prevention) and Sensitized to Acrylates (Secondary Prevention).
| 1. Never touch the polish, especially while it is still soft (non-touch technique). |
| 2. Avoid contact with any products that contain acrylates or have been “contaminated” by acrylates: work “like a surgeon,” keeping these contaminated products at the work station. |
| 3. Try not to contaminate anything. Keep any objects you will touch later (mobile telephones, beverages, door handles, etc.) away from the work station. |
| 4. Always change the manicure station's protective covering after each customer. |
| 5. Nail files, orange wood cuticle sticks, and any other materials used in nail procedures involving polish containing acrylates should not subsequently be used in conventional manicures because they may be contaminated by acrylates and can expose both the manicurist and the customer to these substances. |
| 6. Make sure acrylates are properly cured: All of the customer's nails must remain under the curing lamp for the required period of time. The entire hand must be placed under the lamp. Afterwards, the thumb must be placed under the lamp separately. If the thumb is not cured separately, complete polymerization of the outer half of the thumbnail will not be achieved and the customer will come into contact with traces of sensitizing polymers. Lamp maintenance is also essential: light bulbs must be changed regularly. |
| 7. Hands should be protected with Silvershield/4H gloves (Honeywell Safety Products EMEA, Roissy, France). Finger guards can be cut from gloves to cover the fingers most exposed and affected. These gloves can be purchased through companies that sell clothing and personal protective equipment for workers. Nitrile gloves should be placed over the finger guards to keep them in place and improve protection. These gloves should be changed after each customer. The finger guards can be reused (Fig. 4). |
| 8. It is also advisable to use a mask and protective eyewear. |
| 9. Other uses of acrylates: medical devices (contact lenses, intraocular lenses, dental prostheses, composite fillings, bone cement, insulin pumps, hearing aids, etc.); electrical insulation; compact discs; paint; glue and other adhesives; printer ink; disposable diapers; sanitary napkins; incontinence pads; bandages; etc. |
Most sensitized beauticians can continue to work without developing lesions if they take appropriate protection measures, as described in Table 3. Sensitized consumers and beauticians should avoid the use of any nail care technique involving acrylates. The application of artificial nails is the only exception. This technique involves the use of adhesives containing cyanoacrylate, for which cross-reactions with other acrylates have not been reported. Alternatively, conventional nail polish can be used. Information should also be provided about other sources and uses of acrylates (fillings, prostheses, intravascular procedures, adhesives, etc.).
ConclusionsPermanent nail polish has become very popular because it is quick, affordable, and achieves a good cosmetic result with long-lasting effects. The popularity of these products—combined with a lack of training among beauticians—is leading to a new epidemic of ACD.
Permanent nail polish and curing lamps are sold to the general public in stores and online. Many consumers of various ages have therefore started using these products indiscriminately in their own homes. In the near future, it is quite possible that we will see an increase in the number of acrylate-sensitized “amateur beauticians” due to the ready availability of these products.
Unfortunately, these substances are used for many other purposes. Therefore, sensitization triggered by a purely cosmetic procedure can end up having an impact on the patient later in life. The prognosis of sensitized patients in relation to exposure to other acrylates—especially those used for medical purposes—is unknown. Isolated cases of ACD reactions to fillings and rejection of orthopedic prostheses have been reported in patients who became sensitized through contact with acrylates in permanent nail polish and other nail care procedures.20,25–27 Contraindication of the use of these materials in the future may depend on the following factors: the nature of the molecules that the patient is sensitized to and the molecules she subsequently comes into contact with; the source of exposure; and the length of time the polymer remains in the gel phase before curing completely.
In conclusion, we believe that beauticians should be required to receive adequate training before working in this field. We also believe that the authorities should ban the indiscriminate sale of permanent nail polish kits for domestic use.
For dermatologists who study contact allergy, the most important challenge posed by these patients is to gain an accurate understanding of the consequences of sensitization as it relates to other sources of exposure to acrylates in the short and long term.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Gatica-Ortega ME, Pastor-Nieto MA, Silvestre-Salvador JF. Dermatitis alérgica de contacto por acrilatos en esmaltes permanentes. Actas Dermosifiliogr. 2018;109:508–514.


