

Papulopustular rosacea is a chronic inflammatory disease characterized by erythematous, papular, and papulopustular lesions on the face with variable ocular involvement. Various antimicrobial treatments such as erythromycin, metronidazole, permethrin, and oral tetracyclines have proven effective, as well as topical immunomodulators and, in severe cases, oral isotretinoin.1 However, despite the varied therapeutic arsenal available, rosacea can be difficult to treat in some patients.
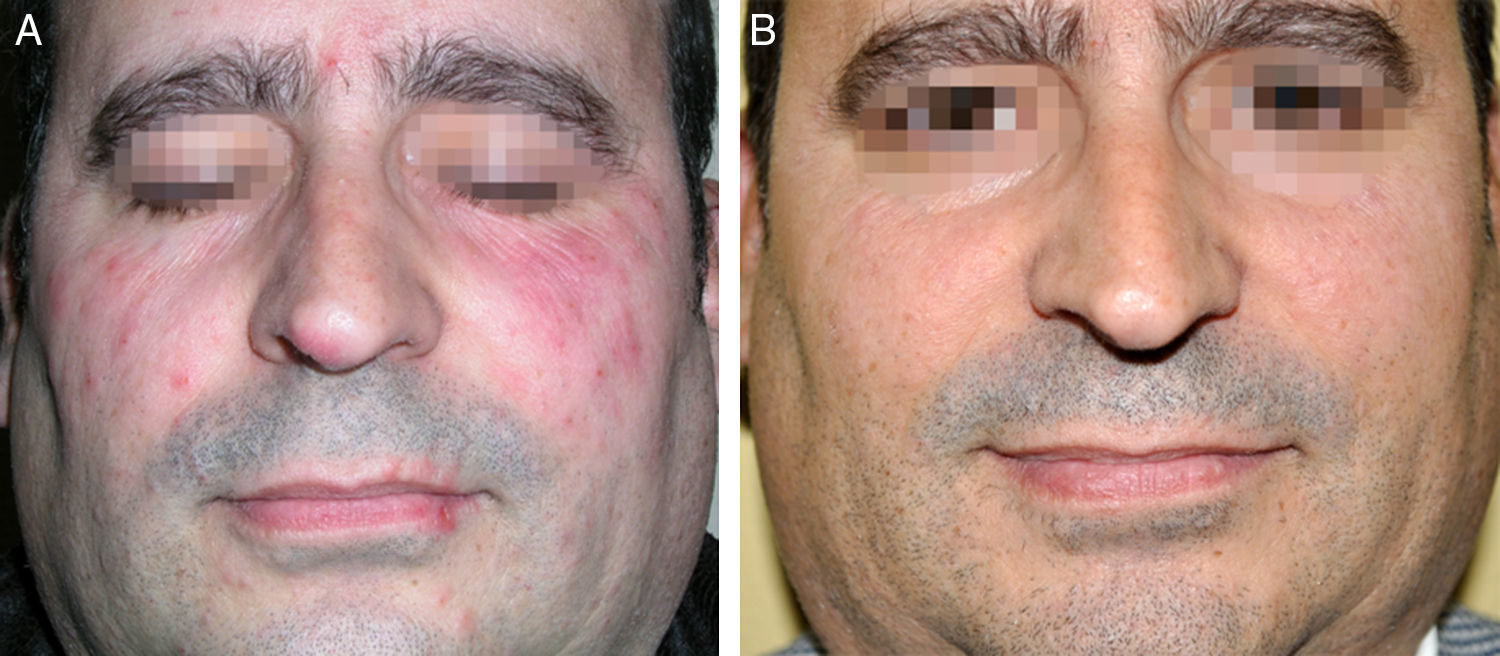
Our patient was a 44-year-old man who had had facial rosacea since age 30 years and no other past history of interest. Over the course of his illness, the patient had received treatment with retinoids and topical immunomodulators, oral cloxacillin, and repeated cycles of doxycycline, with only partial and/or transient improvement. Physical examination revealed diffuse erythema and a moderate number of papuloerythematous lesions on both cheeks and the dorsum of the nose (Fig. 1A). After obtaining informed consent from the patient, we recommended treatment with a single 250μg/kg dose of oral ivermectin and specifically instructed the patient not to apply any topical treatment. After 2 weeks, significant improvement was observed and the disease has remained in complete remission for 6 months after treatment (Fig. 1B).
. B, Clinical appearance 6 months later.")
The etiology and pathogenesis of rosacea is not fully understood. It is thought to be caused by a combination of factors, including augmented immune response, neuroimmune dysregulation, and vasoregulatory alterations.2 There is growing evidence that Demodex mites play a role in the etiology and pathogenesis of rosacea. The density of Demodex organisms has been found to be greater in areas affected by rosacea than in healthy skin, and these mites have been found in a significant proportion of patients with rosacea.3 Good response to acaricidal agents has been reported.1 In addition, Demodex mites have started to gain recognition as one of the numerous factors that trigger the expression of Toll-like receptors 2 (TLR-2), giving rise to the exacerbated immune response observed in patients with papulopustular rosacea.3 Ivermectin is an antiparasitic agent that has been widely used since 1988 for oral treatment of filariasis and other parasitic infections. Ivermectin not only has an antiparasitic effect but also has an immunomodulatory and anti-inflammatory effect by inhibiting the lipopolysaccharide-induced production of cytokines.4 The use of topical ivermectin for the treatment of rosacea was approved by the US Food and Drug Administration in 2014 and by the European Medicines Agency in 2015. Oral ivermectin has also been successfully used, without formal indication, in the treatment of demodicosis, in both immunosuppressed5 and immunocompetent patients.6 Oral ivermectin has also been used, with satisfactory results, in 2 healthy patients with papulopustular rosacea; in 1 case, the patient received 3mg/d for 8 days in association with 5% topical permethrin 3 times a week,7 and in the other case, a child with severe oculocutaneous rosacea received a single dose of 250μg/kg.8
Rosacea can be treated but not cured. Like all chronic diseases, rosacea requires safe, effective treatment that achieves long periods of remission. In patients who have received oral ivermectin for the treatment of systemic infections, adverse effects have been very rare (<1%) over the past few decades and appear to be related to parasite load.9 Similarly, no serious adverse effects have been reported when a single dose (200μg/kg) has been given for the treatment of scabies.1 However, only short-term safety studies have been carried out and it is not known whether repeated treatment is safe. Our patient had no adverse effects and prolonged remission was achieved with a single dose, but prospective studies with large groups of patients are needed in order to confirm our results.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Hernández-Martín Á. Tratamiento con ivermectina oral en un paciente inmunocompetente con rosácea pápulo-pustulosa. Actas Dermosifiliogr. 2017;108:685–686.



