

Solitary fibrous tumor (SFT) is a mesenchymal tumor that typically arises in the pleural cavity. Extrapleural locations, such as the skin, are rare.1 Cutaneous SFT, alongside dermatofibrosarcoma protuberans (DFSP), spindle cell lipoma, dendritic fibromyxolipoma, and superficial acral fibromyxoma, forms part of the family of spindle cell tumors that express CD34.2,3
A 44-year-old woman presented with a slow-growing lesion in the right inguinal region that had been present for 2 years. Physical examination revealed a firm pedunculated tumor with a wide base measuring 1.2cm in diameter. The tumor was excised.
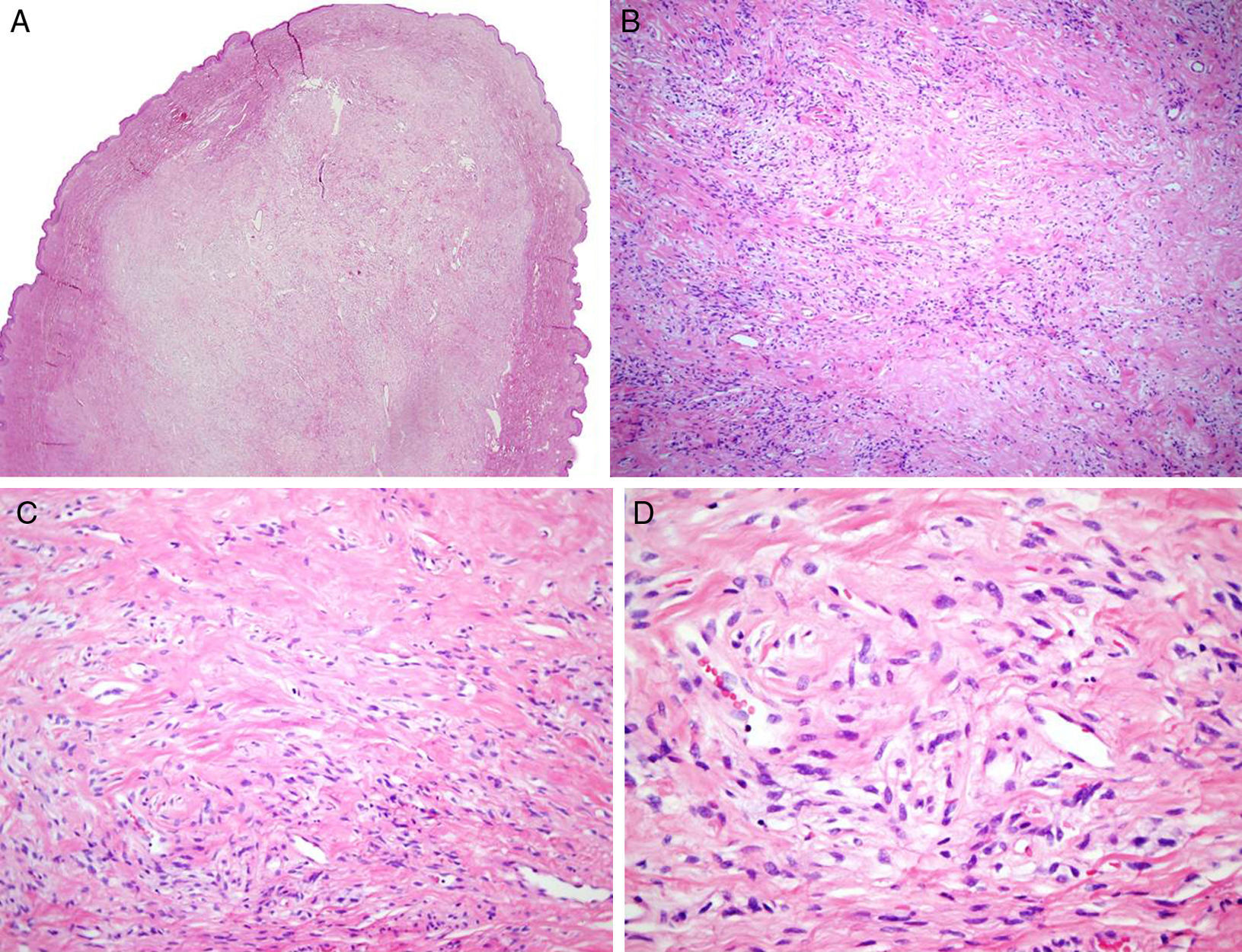
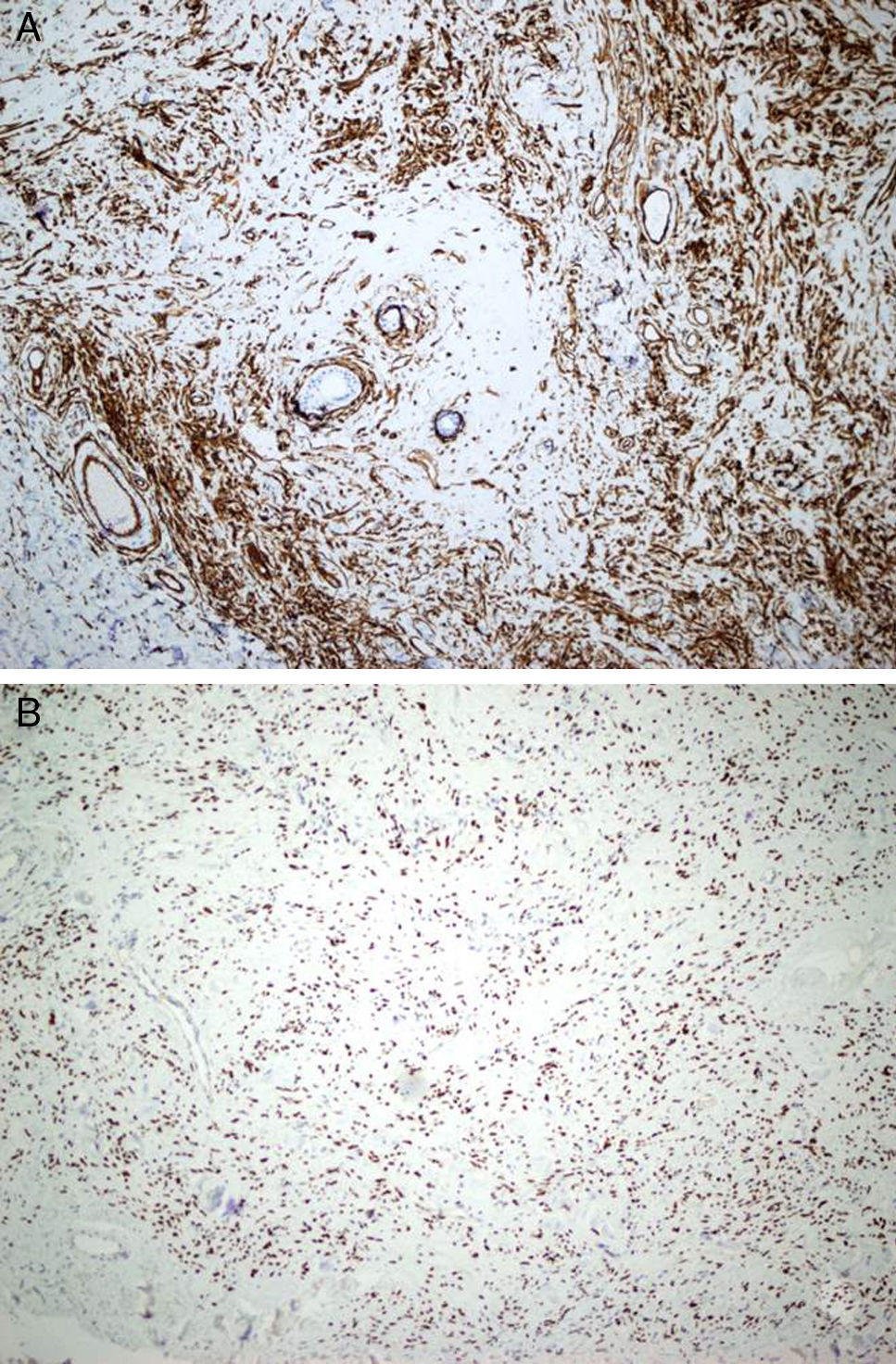
Histopathologic examination showed a polypoid, nonencapsulated lesion with a well-circumscribed dermal proliferation of variable cellular density composed of monomorphic, elongated, oval cells lacking atypia and with scant cytoplasm and no signs of necrosis (Fig. 1A-D). One mitotic figure was identified in 10 high-power fields. Immunohistochemical staining showed positive results for CD34, BCL-2, CD 99, and STAT-6 (Fig. 2 A and B) and negative results for epithelial membrane antigen (EMA), smooth muscle actin (SMA), and S-100 protein. The Ki67 index was 1%.
![A, Polypoid, nonencapsulated lesion with a well-circumscribed dermal proliferation (hematoxylin-eosin, original magnification ×20). B and C, Note the abundant extracellular collagenous matrix in some areas of the tumor (hematoxylin-eosin, original magnification ×100 [A] and ×200 [B]). D, Detail of cells with monomorphic elongated, oval nuclei (hematoxylin-eosin, original magnification ×400).](https://static.elsevier.es/multimedia/15782190/0000010900000002/v1_201803020443/S1578219017304316/v1_201803020443/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w91sAmkCw32Jed9sZf6jzEuDbFpW7G0NfARZs8afh+9K8v8RN+oFy2ZmalFHXVYo6AsHDhAa+d0QOqVxlnfcQbHKZ845aDdgRDbgJPxXOog96f1SFqCorGswZu4LZ7Y0G92fytr91Ss06dYrOv9lTLkzl+dO6rD7byhq/doWwWPUkOm2VP9xHpCNhjv3NsThVaf+dlft5ct6DVLINLv7t2yFDZgPine/peGWlJZB9TmpK1wFNRrOI/1wksgFOoFdn/qhDAPuuwD4zpge0Cg3cjwA= "A, Polypoid, nonencapsulated lesion with a well-circumscribed dermal proliferation (hematoxylin-eosin, original magnification ×20). B and C, Note the abundant extracellular collagenous matrix in some areas of the tumor (hematoxylin-eosin, original magnification ×100 [A] and ×200 [B]). D, Detail of cells with monomorphic elongated, oval nuclei (hematoxylin-eosin, original magnification ×400).")
A, Polypoid, nonencapsulated lesion with a well-circumscribed dermal proliferation (hematoxylin-eosin, original magnification ×20). B and C, Note the abundant extracellular collagenous matrix in some areas of the tumor (hematoxylin-eosin, original magnification ×100 [A] and ×200 [B]). D, Detail of cells with monomorphic elongated, oval nuclei (hematoxylin-eosin, original magnification ×400).
. B, Nuclear staining of Stat 6 (Stat 6, original magnification ×200).")
Cutaneous SFT mainly affects adults, is more common in men (male to female ratio of 4:1), and shows a predilection for the head and neck.1 The most characteristic histopathologic pattern in SFT is a “patternless spindle cell pattern”, with haphazardly arranged spindle cells that do not form a clear storiform, fascicular and/or herringbone, or wavy pattern. The cells are embedded in a collagenous matrix or in amorphous hyaline material, and a hemangiopericytoma-like vascular pattern is often seen in areas of the tumor. Diagnosis is challenging given the variable histopathologic findings. The main entity that should be considered in the differential diagnosis is DFSP. Apart from CD34, SFT expresses vimentin, bcl-2, and CD99 (with positive staining seen in between 40% and 100% of tumors in the case of bcl-2 and CD99). Staining is negative for EMA, SMA, desmin, and protein S-100. CD34 and CD99 positivity may also be observed in DFSP.4,5 One recent study reported that NAB2-STAT6 fusion genes were specific to SFT, indicating that the study of these genes could be of use in overlap cases.2 Nuclear immunostaining with STAT6 has high sensitivity and specificity, with positivity rates ranging from 91% in meningeal SFTs to 100% in soft tissue SFTs.2,6,7 Immunohistochemical markers are important diagnostic tools in cutaneous SFT, and as occurs with SFTs in other locations, STAT6 has a key role in establishing an accurate diagnosis. Distant metastasis has not been observed in cutaneous SFT, but there have been 3 reports of local recurrence.1,8,9 Cutaneous SFT, thus, like its counterparts in other locations, is considered to be a borderline tumor and hence complete surgical excision is recommended.1
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Santos-Juanes J, García-García B, Hidalgo Y, Vivanco B. Tumor fibroso solitario cutáneo: una neoplasia fusocelular con una inmunohistoquímica particular. Actas Dermosifiliogr. 2018;109:183–185.



